Download
1 / 20
200 likes | 423 Views
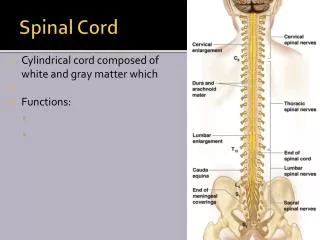
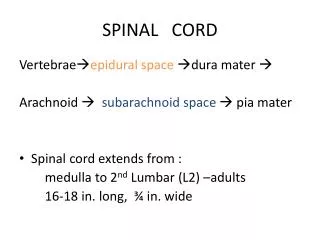
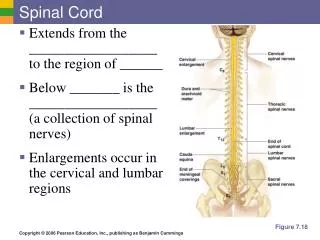
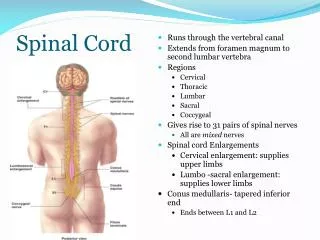
Spinal Cord Disorder. Michael H. Wilhelm, CRNA, APRN. Acute Spinal Cord Injury. Trauma is the leading cause of injury 1.5% to 3.0% cervical spine injury in major trauma 4% to 5% have injury to upper cervical spine C1-C3 Injury can also occur at thoracic and lumbar spinal area.

E N D
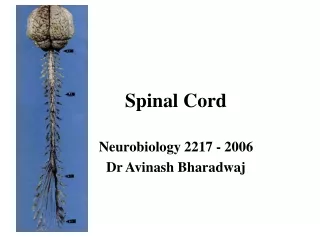
Spinal Cord Disorder Michael H. Wilhelm, CRNA, APRN
Acute Spinal Cord Injury • Trauma is the leading cause of injury • 1.5% to 3.0% cervical spine injury in major trauma • 4% to 5% have injury to upper cervical spine C1-C3 • Injury can also occur at thoracic and lumbar spinal area
Clinical Manifestation • Depend on the extent and level of the injury • Initially • Flaccid Paralysis • Loss of Sensation below level of injury • Classified by the terms of the American Spinal Injury Association
Physiological Effects • Depends on Level of Injury • More severe at cervical level and less sever caudally • Reduction of blood pressure • Loss of sympathetic nervous system activity and a decrease in systemic vascular resistance • Bradycardia resulting from loss of T1-T4 sympathetic innervation to the heart • Can be seen in Thoracic or Lumbar Injury but more common with Cervical Injury • Another Term for these findings is spinal shock • Lasts 1-3 weeks
With Cervical and Thoracic Injury • Major cause or morbdity • Alveolar hypoventilation • Inability to clear secretions • More respiratory muscle impairment with cervical injury • Aspiration of gastric contents • Pneumonia • Pulmonary Embolism
Do we always need an x-ray? • Well Stoelting talks about how x-rays are over used, pt can be evaluated on the following five criteria • No midline cervical spine tenderness • No focal neurologic deficits • Normal sensory • No intoxication • No painful distracting injury
Anesthesia Managment • Airway Management • Special Care with Direct Laryngoscopy • Neck movement minimized • If collar in place have another provider maintain C-Spine immobillization with their hands, document appropriately • If no collor on trauma pt, ensure clearance from trauma team is noted in the chart • Avoid Hypotension • Maintain Spinal Cord Perfusion
More Airway Tips • Other options to Direct Laryngoscopy • Glidescope • Awake FiberopticLaryngoscopy • Pt must be cooperative • Can have visualization problems with blood, secretions and anatomic deformities • Coughing can be detrimental to the pt • Awake Tracheotomy • Only used as a last resort and for the most challenging airways (i.e. facial fractures, deformities) • No matter what method you use always have manual in line stabilization in place
Systemic Systems • Absence of compensatory sympathetic nervous system • Drastic drop in blood pressure can be noted • Changes in body position, blood loss, or positive pressure ventilation • Liberal Intravenous Infusion of crystalloid solution • Fill the intravascular spaces • Acute blood loss should be treated rapidly
EKG changes are common especially with a cervical spine injury • Breathing best managed by ventilator • Loss of accessory muscles • Body Temperature should be maintained and monitored • Pts become poikilothermic below level of injury
GA can be done with anesthetic gases or TIVA • Caution with Nitrous Oxide as it can expand gas in closed spaces • Especially in Basilar Skull Fractire of Rib Fractire • Can worsen a pneumocephalus or a pneumothroax • Arterial hypoxemia is common • Monitor Pulse Oximetry and Oxygen Supplementation
Muscle Relaxation? • Base decision on location of operative site and the level of spinal injury • Pancuromium • Sympathomimetic effects • Succyncholine • No excess potassium release seen with an initial spinal cord injury after a few hours
Chronic Spinal Cord Injury • Anesthesia Focus should be to prevent Autonomic Hyperreflexia • Non-Depolarizing Muscle Relaxant Drugs are the drug of choice • Depolarizing Muscle Relaxants will provoke hyperkalemia • Particularly for the initial 6 months after the injury • Do not use after 24 hours of injury • May see varying of heart rate and blood pressures • Chronic immobile patients should always have a high suspicion of pulmonary thromboemolism • Intercostal Muscle impairment can lead to difficulty in extubation • Impaired Cough and Excessive Secretions • Continue Baclofen and Benzodiazepines to prevent withdrawal symptoms
Autonomic Hyperreflexia • Autonomic Hyperreflexia Syndrome • Associated with the body’s resolution of the effects of spinal shock • Commonly associated with injuries at or above T-6 • Presentation • Sudden hypertension • Bradycardia • Pounding headache • Blurred vision • Sweating and flushing of skin above the point of injury
How do we treat it? • Patients at risk should be treated to prevent stimulation below the lesion, even though no prior history all spinal cord patients are at risk. • Prior to intiating a surgical stimulus • General • Neuraxial • Regional • Use short acting vasodilators to treat hypertention
Spinal Cord Tumors • Anesthesia Management • Area of tumor and size with resulting neurological compromise can vary the treatment needed • Airway Management • Cervical Tumors may obstruct the view of the airway • Severe movement can cause further damage • Avoid hypotension and anemia • Supplemental Oxygen • Maintain spinal cord perfusion and oxygenation • Caution in use of depolarizing muscle relaxants
Intervertebral Disc Disease • Cervical Disc Disease • Lumbar Disc Disease