Download
1 / 45
470 likes | 1.64k Views
INCRETINAS e INHIBIDORES DPP-4 EN DIABETES MELLITUS TIPO 2. Dr. Marco De León Espitia Médico Internista – Intensivista H.U.S. – U.I.S. www.marcodeleon.com. Septiembre 17 de 2010 FHUM Barranquilla. METFORMINA. TIAZOLIDINEDIONAS. CONTROL DE HIPERGLICEMIA. INHIBIDORES DE

E N D
INCRETINAS e INHIBIDORES DPP-4EN DIABETES MELLITUS TIPO 2 Dr. Marco De León Espitia Médico Internista – Intensivista H.U.S. – U.I.S. www.marcodeleon.com Septiembre 17 de 2010 FHUM Barranquilla
METFORMINA TIAZOLIDINEDIONAS CONTROL DE HIPERGLICEMIA INHIBIDORES DE ALFA GLUCOSIDASA SULFONIUREAS ANALOGOS GLP-1 INHIBIDORES DPP-4
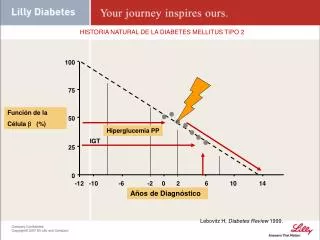
Se ha observado que la administración oral de glucosa produce 50 – 70 % mas de secreción de insulina cuando se compara con una dosis equivalente intravenosa. A este fenómeno se le llama EFECTO INCRETINA. Y es causado por dos hormonas: (GIP) poli péptido insulinotropico dependiente de glucosa (GLP-1) péptido similar al glucagon -1 EL SISTEMA DE INCRETINAS The journal of clinical investigation Vol.46, N° 12, 1967 PERLEY - KIPNIS
Sitagliptina Vildagliptina Saxagliptina Alogliptina DPP4 GLP-1
Incrementa la Liberación de Insulina Disminución del Glucagón en células Alfa pancreáticas Aumenta la saciedad en SNC Estimula el crecimiento e incrementa la supervivencia de las células Beta Pancreáticas. Estimula la proliferación y diferenciación de nuevas células Beta. ACCIONES GLP-1
DPP-4 DipeptidylPeptidasa 4 (CD 26) Es la causante de la rápida degradación de las INCRETINAS. Esta presente en: Riñones - Intestino Hígado - Placenta Útero - Próstata Piel - Endotelio capilar Plasma - Fluidos corporales . La inhibición de la DPP-4 resulta en la prolongación del efecto fisiológico de las incretinas endógenass The American Journal of medicine (2010) 123, S28-S37
SITAGLIPTINA VILDAGLIPTINA SAXAGLIPTINA ALOGLIPTINA INHIBIDORES DE LA DPP-4
SITAGLIPTINA VILDAGLIPTINA Una dosis de 50 – 200 mg produce más de 80 % de reducción de la actividad de la DPP-4, incrementando 2 á 3 veces los niveles de GLP – 1. Excreción urinaria 80 – 90 % Descenso de la HbA1c entre 0.3 – 0.9 % En mono terapia. Y de 0.9 – 1.3 En combinación con otros antidiabéticos orales
SITAGLIPTINA vs. METFORMINA Diabetes, Obesity and Metabolism 12; 252-261, 2010 6 meses Tamizados: n= 2068 Excluidos n = 1018 Aleatorizados n = 1050 Sitagliptina 100 mg q.d. N = 528 Metformina 1.000 mg b.i.d n = 522
SITAGLIPTINA vs. METFORMINA Diabetes, Obesity and Metabolism 12; 252-261, 2010
SITAGLIPTINA vs. METFORMINA Diabetes, Obesity and Metabolism 12; 252-261, 2010
SITAGLIPTINA + METFORMINA vs. Mono terapias (SIT. – MET.) Diabetes Care, Vol. 30, N° 8, 1979 - 1987 August 2007 24 semanas N = 1091 (P) = 165 (M 1000 mg) = 178 (M 2000 mg) = 177 (S 50 mg + M 2000 mg) = 178 (S 100 mg) = 175 (S 50 mg + M 1000 mg) = 183
SITAGLIPTINA + METFORMINA vs. Mono terapias (SIT. – MET.) Diabetes Care, Vol. 30, N° 8, 1979 - 1987 August 2007 Metformina 500 mg b. i. d. Sitagliptina 50 mg + Metformina 1000 mg b. i. d. Placebo Sitagliptina 50 mg + Metformina 500 mg b. i. d. Sitagliptina 100 mg q. d. Metformina 1000 mg b. i. d.
SITAGLIPTINA + METFORMINA vs. Mono terapias (SIT. – MET.) Diabetes Care, Vol. 30, N° 8, 1979 - 1987 August 2007 Metformina 500 mg b. i. d. Sitagliptina 50 mg + Metformina 1000 mg b. i. d. Placebo Sitagliptina 50 mg + Metformina 500 mg b. i. d. Sitagliptina 100 mg q. d. Metformina 1000 mg b. i. d.
SITAGLIPTINA + Insulina vs. Insulina Sitagliptina 100 mg día q. d. Más insulina N = 322 Placebo Más insulina N = 319 24 semanas – Multicentrico – Doble ciego – Randomizado – 100 centros clínicos Diabetes Obesity and Metabolism 12; 167 – 177, 2010
SITAGLIPTINA + Insulina vs. Insulina Diabetes Obesity and Metabolism 12; 167 – 177, 2010
SITAGLIPTINA + Insulina vs. Insulina Diabetes Obesity and Metabolism 12; 167 – 177, 2010
VILDAGLIPTINA Diabetes research and clinical practice 76 (2007) 132 – 138. 24 semanas – doble ciego – Aleatorizado – Multicentrico – Controlado N = 354 Vildagliptina 50 mg día N = 88 Vildagliptina 50 mg b. i. d. N = 83 Vildagliptina 100 mg día N = 91 Placebo N = 92
VILDAGLIPTINA Diabetes research and clinical practice 76 (2007) 132 – 138.
VILDAGLIPTINA Diabetes research and clinical practice 76 (2007) 132 – 138.
VILDAGLIPTINA + METFORMINAVS. Metformina Diabetes care 30: 8090 – 895, 2007 Doble ciego – Aleatorio - Multicentrico 24 semanas Vildagliptina 50 mg Metformina 1500 mg N = 177 Vildagliptina 100 mg dia Metformina 1500 mg dia N = 185 Pacebo Metformina 1500 mg dia N = 182
VILDAGLIPTINA + METFORMINAVS. Metformina Diabetes care 30: 8090 – 895, 2007 Vildaglip. 50 mg día Vildaglip. 100 mg día Placebo
VILDAGLIPTINA + METFORMINAVS. Metformina Diabetes care 30: 8090 – 895, 2007 Vildaglip. 50 mg día Vildaglip. 100 mg día Placebo
VILDAGLIPTINA + Insulina vs. Insulina Vildaglitina + insulina N = 144 Placebo + insulina N = 152 24 semanas – Controlado – Randomizado – Doble ciego Grupo control con placebo – 50 mg cada 12 horas Diabetología (2007) 50: 1148 - 1155
VILDAGLIPTINA + Insulina vs. Insulina INSULINA INSULINA + VILDAGLIPTINA Diabetología (2007) 50: 1148 - 1155
VILDAGLIPTINA+ METFORMINA GLICLAZIDA+ METFORMINA VS. Journal compilation – Diabetes medicine 2010 – 27; 318-326
VILDAGLIPTINA+ METFORMINA GLICLAZIDA+ METFORMINA VS. Journal compilation – Diabetes medicine 2010 – 27; 318-326
VILDAGLIPTINA+ METFORMINA GLICLAZIDA+ METFORMINA VS. Journal compilation – Diabetes medicine 2010 – 27; 318-326
EFECTOS SECUNDARIOS inh. DPP-4 No presentan influencia sobre el peso corporal. J. Am. Pharm. Assoc. 2009: 49 (suppl 1) : S16 – S29.
Total participantes n= 104 Manejo convencional + Intervención dietaría (n=45) Manejo convencional (n= 48) BMJ 2010; 341: c3337
N = 405 < 75 años No controlado Intervención en estilos de vida 12 semanas TT0. Oral sin insulina DIABETES TECHNOLOGY & THERAPEUTICS Vol. 12, N° 7, 2010
COMPARACION ENTRE ANALOGOS DE INCRETINAS (Exenetide) vs. INHIBIDORES DPP-4 (Sitagliptina) The American Journal of Medicine (2010) 123, S28 – S37
DPP-4 CONCLUSIONES 1 La evidencia actual señala el uso de Los inhibidores DPP-4 en combinación Con otros hipoglucemiantes orales o insulina Para obtener su mayor beneficio.
DPP-4 CONCLUSIONES 2 La mas importante y eficaz estrategia de lucha Contra las enfermedades metabólicas y sus Riesgos implícitos, sigue siendo el ESTILO DE VIDA SALUDABLE (alimentación, actividad física, IMC)
DPP-4 CONCLUSIONES 3 HACEN FALTA ESTUDIOS INDEPENDIENTES QUE MUESTREN A LARGO PLAZO EL VERDADERO IMPACTO DE LOS INHIBIDORES DPP-4 y LOS ANALOGOS DE INCRETINAS EN LA SOBREVIDA DE LOS PACIENTES DIABETICOS y SUS COMPLICACIONES CRONICAS
DPP-4 CONCLUSIONES 4 Tanto el medico general como el especialista Tienen el deber ético y académico de evaluar En detalle, con asertividad, Sensatez, prudencia y juicio Clínico responsable los tan de moda: ESTUDIOS DE NO INFERIORIDAD, antes de ofrecer novedosas alternativas terapéuticas a sus pacientes.
DPP-4 CONCLUSIONES 5 EN LA AMPLIA GAMA DE OPCIONES TERAPEUTICAS QUE OFRECE ACTUALMENTE EL MERCADO FARMACOLOGICO PARA LA DIABETES MELLITUS, EL MEDICO DEBE INDIVIDUALIZAR LA ESCOGENCIA BASADO EN CONSIDERACIONES ESTRICTAMENTE FISIOLOGICAS QUE DERIBEN DEL CONOCIMIENTO AMPLIO y SUFICIENTE DE LAS MOLECULAS A USAR.
GRACIASpor su atención WWW.MARCODELEON.COM “Si la falsedad, como la verdad, tuviese un solo rostro, estaríamos mejor, ya que podríamos considerar cierto lo opuesto de lo que dijo el mentiroso. Pero lo contrario a la verdad tiene mil formas y un campo ilimitado.” Montaigne