Download
1 / 30
300 likes | 486 Views
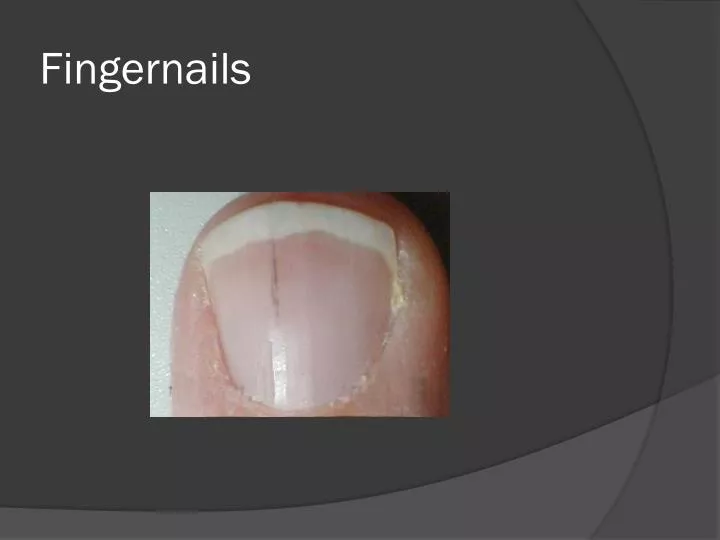
Fingernails. Conjunctiva. Skin. CT ABDOMEN. MRI BRAIN. Infective Endocarditis. Duke Criteria. Definative: 2 major, 1 major and 3 minor, 5 minor Possible: 1 major and 1 minor OR 3 minor crieria met. Duke Criteria. Major: Positive Blood culture: Evidence of endocardial involvement.

E N D
Duke Criteria • Definative: 2 major, 1 major and 3 minor, 5 minor • Possible: 1 major and 1 minor OR 3 minor crieria met
Duke Criteria • Major: • Positive Blood culture: • Evidence of endocardial involvement
Duke Criteria – Major • Positive Blood culture: • Typical microorganism for infective endocarditis from two separate blood cultures • Viridans Streptococci, streptococcus bovis, HACEK group, staph aureas, Community acquired enterococcus in absence of a primary focus OR • Persistently positive blood culture (3/4 cultures or 2 cultures >12 hours apart) • Single positive for coxiella bunetti, or phase I IgG titer of >1:800
Duke Criteria – Major • Endocardial Involvement • Positive Echo: • Oscillating intracardiac mass on valve or supporting structures in the path of regurgitant jet or in implanted material in the absence of an alternative anatomic explanation • Abscess • New partial dehiscence of prosthetic valve • New Valvular Regurgitation • Increase or change in previous murmur not sufficient
Duke Criteria – Minor • Predisposing condition • Abnormal valve (prior endocarditis, rheumatic valvular disease, Aortic Valvular disease, complex cyanotic lesions, prosthesis • Abnormal risk (IVDU, indwelling catheters, poor dentition, hemodialysis, DM • Fever ≥38.0 C • Vascular Phenomena: • Major arterial emboli, septic pulmonary infarctions, mycotic aneurism, intracranial hemorrhage, conjunctival hemorrhages, Janeway lesions
Duke Criteria – Minor • Immunologic Phenomena: Glomerulonephritis, Osler;s nodes, Roth’s sports, rheumatoid factor • Microbiologic evidence: • Positive blood culture but not meeting major criteria • Usu: gnr’s • Serologic evidence of active infection with organism consistent with infective endocarditis
IE - Acute vs. Subacute • Acute • More virulent pathogen • Rapid valvular damage • Rapid hematogenous seeding of extracardiac sites • Untreated leads to death in days to weeks • Typical exam findings of vascular phenomenon: Janeway lesions, emboli, mycotic aneurisms
IE - Acute vs. Subacute • Acute Organisms • Staphylococcus Aureas (MRSA and MSSA) • Beta Hemolytic Streptococcus • Pneumococcus • Enterococcus, Coag negative Staph (less commonly)
IE - Acute vs. Subacute • Subacute • Indolent course. • gradual valvular damage • Rarely has seeding of extracardiac sites • Generally has more signs of rhematologic activation: roth spots, RF+, osler’s nodes, GN
IE - Acute vs. Subacute • Subacute Organisms • Viridan’s Streptococcus • Enterococci • Coagulase negative Staph • HACEK • haemophilus ssp., • actinobaciullus actinomycetemcomitans, • cadiobacterium hominis, • eikenella corrodens, • kingella ssp. • Strep Bovis with colon cancer.
Cardiac Complications • CHF – 30-40% • Consequence of valvular disease • Perivalvular Abscess • Perivalvular fistula • Pericarditis • Varying degrees of heart block • Mitral: may interrupt the AV node, or bundle of his • Aortic: non-cardiac or right sinus: upper interventricular system.
Extra-cardiac Findings • Musculoskeletal • Septic and reative arthritis, bone infarctions, back pain, • Skin • Subungual hemorrhages, janeway lesions, osler’s nodes, • Eyes: • Roth’s spots, conjunctivalpetichiae, • Neuro: • CVA in up to 40%, aseptic and purulent meningitis, intracranial hemorrhage, seizures, encephalopathy, microabscesses in brain and meninges, • Renal: • Immune complex deposition in GBM, embolic infarcts, abscesses • Embolic: • Any organ can be involved but most often are skin, kidneys, spleen, skeletal system, brain and meninges
Treatment • Medical Management: • Difficult to eradicate bacteria from the valve. • Should use long course of IV bacteriocidal antibiotics and static antibiotics should be avoided. • Antibiotic management should be held for cultures to be drawn. • Either 4 over the course of an hour, or 2 and 2 12 hours apart. • Even with appropriate management some may continue to spike fevers and have + BC
Treatment – Medical Mgmt. • Strep ssp.: • Pen sensitive: Penicillin G, ceftriaxone, vanc for 4 wks, OR penicilin/ceftr plus gent for 2 weeks • Pen resistant: Penicillin G plus gent for 4-6wks OR Vanc 4 weeks • Enterococcus: • Pen g plus gen for 4-6 weeks, OR Amp plus gent for 4-6 weeks, OR vank plus gent for 4-6 weeks • HACEK: • Ceftriaxone for 4 weeks OR Amp/Sulbactam 4 weeks
Treatment – Medical Mgmt. • MRSA • Native valve • Vanc for 4-6 weeks • Prosthetic valve • Vanc plus gent plus rifampin for 6-8 weeks • MSSA • Native valve • Naf/oxacillin/cefazolin 4-6 wks plus gent for 4-5 days, OR vanc for 4-6 weeks • Prosthetic valve • Naf/oxacillin for 6-8 weeks plus gent for 2 weeks plus rifampin for 6-8 weeks
Treatment – Surgical • When to consider surgical therapy • Emergent (same day): • aortic reguritation and preclosure of mitral valve • sinus of valsalva abscess rupture into right heart • rupture into pericardial sac
Treatment – Surgical • Urgent (1-2 days): • Valve obstruction by vegitation • Unstable prosthesis • Ao regurgitation with NYHA 3-4 CHF • Septal perforation • Perivalvular infection • Lack of effective antibiotic therapy • Major embolus plus persisting large vegetation (evidence conflicting but concensus opinion)
Treatment – Surgical • Elective (earlier usually preferred): • Progressive paravalvular prothetic regurgitation • Valve dysfuntion plus persistent infection after 7-10 days of Abx • Fungal endocarditis (specifically mold) • Prosthetic vave: • With staph • <2 moths after preplacement • Fungal • Antibiotic resistant
Treatment – Surgical • Abx after surgery: • If native valve and uncomplicated with negative valve cultures: • 2 weeks of post operative antibiotics OR a total full duration of above regimen whichever is longer • If complicated by perivalvular abscess, partially treated prosthetic valve infection or cases with culture positive valves: • Full course of antibiotics after surgery
Complication rate: • Mortality with staph aureas: 70% with medical management - decreases to 25% with surgical intervention • Splenic abscess 3-5% • Should be treated with drain placement • Mycotic aneurisms: 2-15%, 50% in cerebral vasculature • Some resolve with Abx so monitor with cerebral angiography recommended • Persistent enlarging or periferal aneurisms should be resected surgically if possible • Vegitations • 50% remain unchanged 3 months after cure is achieved, and 25% have slight improvement
Prophylaxis: • Indications: • Prosthetic heart valves • Prior endocarditis • Unrepaired cyanotic congenital heart disease • Completely repaired congential heart disease <6 months after repair) • Incompletely repaired congenital heart diease with residual defects adjacent to prosthetic material • Valvulopathy developing after cardiac transplantation
Prophylaxis: • Regimens: • Standard: amoxicillin 2.0 g PO 1 hour prior to procedure • If pen allergic: • clarithromycin or azithro 500 mg prior to procedure • Cefalexin 2.0 g PO prior to procedure • Clindamycin 600 mg prior to procedure
Bibliography • Durack DT, Lukes AS, Bright DK. New criteria for diagnosis of infective endocarditis: utilization of specific echocardiographic findings. Duke Endocarditis Service. American Journal of Medicine. 96(3):200-9, 1994. • Jennifer S. Li, Daniel J. Sexton, Nathan Mick, Richard Nettles, Vance G. Fowler, Jr., Thomas Ryan, Thomas Bashore, G. Ralph Corey . Proposed Modifications to the Duke Criteria for the Diagnosis of Infective Endocarditis. Clinical Infectious Diseases, Vol. 30, No. 4 (Apr., 2000), pp. 633-638 • Kasper DL, Braunwald E, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J. (2008). Harrison's principles of internal medicine (17th ed.). Pp.789-798; New York: McGraw-Hill Medical Publishing Division • Fuster, O’rourke, Walsh, Poole-Wilson. (2008). Hurst’s The heart Manual of Cardiology (12th ed.). 1975-2004. New York: McGraw-Hill Medical Publishing Division