Download
1 / 63
630 likes | 753 Views
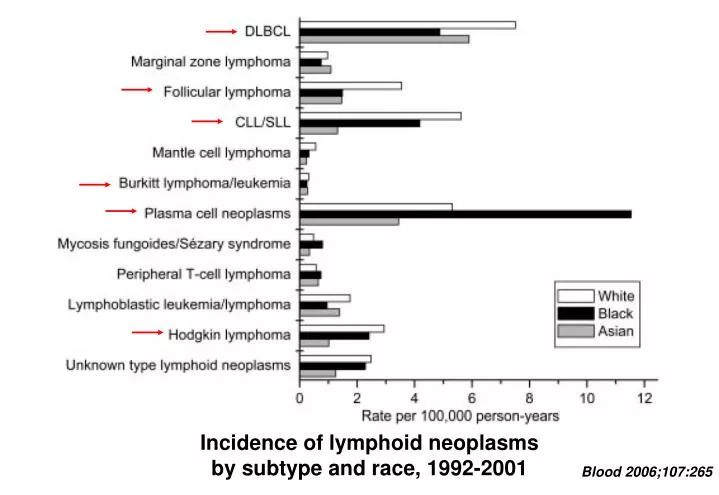
Incidence of lymphoid neoplasms by subtype and race, 1992-2001. Blood 2006;107:265. CHRONIC LYMPHOCYTIC LEUKEMIA. 25-30% of all leukemia in Western Hemisphere Rare at age < 40; incidence rises with age B-cell phenotype

E N D
Incidence of lymphoid neoplasms by subtype and race, 1992-2001 Blood 2006;107:265
CHRONIC LYMPHOCYTIC LEUKEMIA 25-30% of all leukemia in Western Hemisphere Rare at age < 40; incidence rises with age B-cell phenotype About half of cases resemble “naïve” B-cells, half have post-germinal center phenotype with mutated Ig Vh gene Unmutated Ig Vh gene associated with worse prognosis Dx: persistent, absolute lymphocytosis in blood & marrow Confirm clonal B-cell population via flow cytometry Most patients have diffuse lymph node involvement
Incidence of CLL/SLL by race, sex, and age, 1992-2001 Blood 2006;107:265
CHRONIC LYMPHOCYTIC LEUKEMIA Smudge cell Blood smear Nodular marrow infiltration Packed marrow
COMPLICATIONS CHRONIC LYMPHOCYTIC LEUKEMIA Constitutional symptoms (fatigue) Anemia, thrombocytopenia Progressive lymph node enlargement Other organ infiltration Infection (bacteria, fungi, zoster, Pneumocystis) Autoimmune hemolysis/thrombocytopenia Transformation to aggressive lymphoma Other solid tumors (skin, lung, GI most common)
CHRONIC LYMPHOCYTIC LEUKEMIATreatment options • Chlorambucil (25-35% overall response, 2-10% CR) • Cytoxan, vincristine, prednisone (CVP) • Nucleoside analogs (fludarabine, cladribine) • Response rates higher than chlorambucil but overall survival similar; somewhat more toxic • Rituximab, other immunotoxins • More aggressive chemotherapy for refractory disease • IVIG for hypogammaglobulinemic patients with recurrent infection • No advantage to treating asymptomatic disease
Fludarabine Compared with Chlorambucil as Primary Therapy for Chronic Lymphocytic Leukemia NEJM 2000;343:1750 Event-free survival Overall survival
Fludarabine Compared with Chlorambucil as Primary Therapy for Chronic Lymphocytic Leukemia NEJM 2000;343:1750
FLUDARABINE WITH SEQUENTIAL OR CONCURRENT RITUXIMAB IN PREVIOUSLY UNTREATED, SYMPTOMATIC CLL Blood 2003;101:6 Event free survival Overall survival
BIOLOGY NON-HODGKINS LYMPHOMA Often associated with chromosome translocations linking oncogene with immunoglobulin gene (B-cell phenotypes) or T-cell receptor gene (T-cell phenotypes) Etiology: EBV, HTLV-1 Immunodeficiency states Environmental (pesticides, etc) Familial predisposition
CLASSIFICATION NON-HODGKINS LYMPHOMA "Favorable" (indolent) Intermediate High-grade (aggressive)
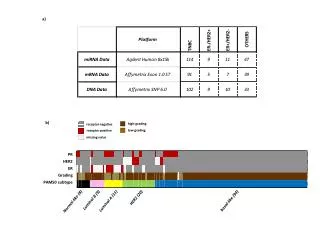
INFORMATION USED IN CLASSIFICATION NON-HODGKIN'S LYMPHOMA Morphology Immunohistochemistry Immunophenotype (flow cytometry) Cytogenetics Molecular features (gene expression, etc) Clinical setting Pattern of spread
Low-grade non-Hodgkin’s lymphomas Small lymphocytic lymphoma/CLL Follicular lymphoma
Intermediate- and high-grade non-Hodgkin’s lymphomas Large B-cell lymphoma Burkitt’s lymphoma
"FAVORABLE" SUBTYPES NON-HODGKINS LYMPHOMAS Follicular (nodular) or diffuse histology Small, well-differentiated cells or small cleaved cells Primarily B-cell phenotype Slow growth Usually advanced stage at presentation Asymptomatic patients may not need Rx Often good response to initial treatment High relapse rate (? incurable) but prolonged survival possible
FOLLICULAR LYMPHOMA • About 20% of all non-Hodgkin’s lymphoma • Median age about 60; rare in young people • Usually presents with widespread disease • <20% stage I, 50% stage IV; 40-50% have marrow involvement • Typically CD20+, CD5-, CD10+ • t(14;18), overexpression of BCL-2 oncogene
Incidence of follicular NHL by race, sex, and age, 1992-2001 Blood 2006;107:265
SURVIVAL IN FOLLICULAR LYMHOMA J Clin Oncol 23:5019-5026
NON HODGKINS LYMPHOMATreatment options for low grade disease • Low dose alkylators (chlorambucil) • Cytoxan, vincristine, prednisone (CVP) • Nucleoside analogs (fludarabine, cladribine) • Rituximab, other immunotoxins • Local XRT • More aggressive chemotherapy/ABMT for refractory/transformed disease • No advantage to treating asymptomatic disease
Immediate treatment vs watchful waiting in asymptomatic patients with advanced stage low-grade NHL Lancet 2003;362:516
CVP vs R-CVP in Advanced Follicular Lymphoma Blood 2005;105:1417
INTERMEDIATE SUBTYPES NON-HODGKINS LYMPHOMAS Diffuse histology (> 90%) Large cells or small cleaved cells B-cell or T-cell phenotype Moderate growth rates May present in extranodal sites 40-50% curable with combination chemotherapy
Diffuse large cell lymphoma • About 30% of NHL • Median age about 65; can occur in young people • About equal proportions of localized and disseminated disease at presentation. Often involves extranodal tissue • CD20+ • t(14;18), t(8;14), t(3;14) • Oncogenes: BCL-2, C-MYC, BCL-6
Incidence of B-large cell lymphoma by race, sex, and age, 1992-2001 Blood 2006;107:265
Comparison of a Standard Regimen (CHOP) with Three Intensive Chemotherapy Regimens for Advanced Non-Hodgkin's Lymphoma NEJM 1993;328:1002 Time to treatment failure Overall survival
CHOP vs CHOP + rituximab in elderly patients with large B-cell lymphoma J Clin Oncol 2005;23:4117 Event-free survival Overall survival
Event-free survival All patients “High intermediate” risk pts Initial Treatment of Aggressive Lymphoma with High-Dose Chemotherapy and Autologous Stem-Cell Support N Engl J Med 2004;350:1287
AGGRESSIVE SUBTYPES NON-HODGKINS LYMPHOMA Blastic morphology "small non-cleaved" = Burkitt's lymphoblastic Propensity for marrow, blood, CNS involvement Rapid growth Cure possible with aggressive combination chemotherapy
BURKITT LYMPHOMA • <1% of NHL • Median age 31; some cases in children • Same as L3 ALL • Most present with localized disease, about 40% with disseminated disease. Extranodal involvement common (up to 80% of pts) • Very fast-growing, most have high LDH • CD20+, CD10+, CD5-, tdT- • t(8;14), t(2;8), t(8;22) with overexpression of C-MYC
Incidence of Burkitt lymphoma by race, sex, and age, 1992-2001 Blood 2006;107:265
NON-HODGKINS LYMPHOMA: SURVIVAL VS TIME 100 % SURVIVING INTERMEDIATE & HIGH GRADE LOW GRADE 0 10 yrs
Survival patterns in NHL - 1 ALCL, anaplastic large T/null-cell lymphoma; MZ, MALT, marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue; FL, follicular lymphoma Blood 1997;89:3909-3918
Survival patterns in NHL - 2 MZ, nodal, marginal zone B-cell lymphoma of nodal type; LP, lymphoplasmacytoid lymphoma; SL, small lymphocytic lymphoma Blood 1997;89:3909-3918
Survival patterns in NHL - 3 Med LBC, primary mediastinal large B-cell lymphoma; DLCBL, diffuse large B-cell lymphoma; HG, BL, high-grade B-cell Burkitt-like lymphoma Blood 1997;89:3909-3918
Survival patterns in NHL - 4 T-LB, precursor Tlymphoblastic lymphoma; PTCL, peripheral T-cell lymphoma; MC, mantle cell lymphoma. Blood 1997;89:3909-3918
HODGKIN’S DISEASE Cervical lymphadenopathy Hilar and mediastinal lymphadenopathy
Hodgkin’s disease: Reed-Sternberg cell (blue arrow) and Hodgkin’s cell (red arrow) in marrow biopsy
NEJM 2003; 349:1324 EPIDEMIOLOGY HODGKIN'S DISEASE Annual incidence in US: 5-7 cases/100,000 persons Median age approx 30 yrs Bimodal age distribution More common in upper socioeconomic strata Role of EBV in pathogenesis
Incidence of Hodgkin lymphoma by race, sex, and age, 1992-2001 Blood 2006;107:265
BIOLOGY HODGKIN'S DISEASE Virtually all cases originate in lymph nodes Most present with supradiaphragmatic disease Initial spread to adjacent node groups Immune response to tumor Non-malignant lymphocyte infiltration Fibrosis/sclerosis Constitutional signs
STAGING HODGKIN'S DISEASE I - single node or group of contiguous nodes II - two node groups, same side of diaphragm III - nodes (or spleen), both sides of diaphragm IV - extranodal (other than by direct extension) (liver, marrow, lung most common) "B" symptoms: fever, weight loss, night sweats
HODGKIN’S DISEASE Potential sites of lymphatic spread
TREATMENT HODGKIN'S DISEASE Stage I or IIA: radiotherapy or combined modality (chemo + local XRT) Stage IIB or greater: combination chemotherapy (ABVD, etc) Bulky tumors may require both modalities Cure rates > 70-80% possible
Long-term cause-specific mortality in patients treated for Hodgkins disease J Clin Oncol 2003;21:3431
CLASSIFICATION PLASMA CELL DYSCRASIAS Monoclonal gammopathy of uncertain significance (MGUS) "Benign"/idiopathic Associated with other diseases (autoimmune, infectious, non-heme cancer, etc) Plasma cell or lymphoid malignancy Waldenstrom's macroglobulinemia Other lymphoproliferative disorders Smoldering multiple myeloma Multiple myeloma
Incidence of plasma cell neoplasm by race, sex, and age, 1992-2001 (predominantly multiple myeloma) Blood 2006;107:265