Download
1 / 35
410 likes | 1.6k Views
Transposition of the Great Arteries. Eric Osborn January 27, 2010. Outline. Definitions Embryology Epidemiology Complete transposition (D-TGA) Congenitally corrected transposition (L-TGA) Echocardiography. Definitions.

E N D
Transposition of the Great Arteries Eric Osborn January 27, 2010
Outline • Definitions • Embryology • Epidemiology • Complete transposition (D-TGA) • Congenitally corrected transposition (L-TGA) • Echocardiography
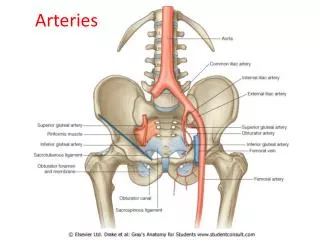
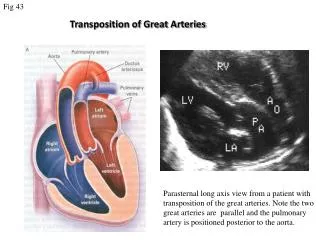
Definitions • The key anatomic characteristic of transposition complexes is ventriculoarterial discordance. • The aorta arises from the morphological RV • The PA arises from the morphological LV
Definitions • Complete transposition (D-TGA) • Atrioventricular concordance
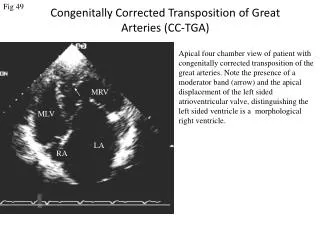
Definitions • Congenitally corrected transposition (L-TGA) • Atrioventricular discordance
Embryology • 22 days gestation … the primitive straight cardiac tube is formed
Embryology • 23 days gestation … the straight cardiac tube elongates and bends forming the cardiac loop. • Cephalic portion bends ventrally, caudally, and right-ward. • Caudal portion moves dorsally, cranially, and left-ward. • The rotational motion folding over of the bulboventricular portion bringing the future ventricles side-by-side.
Embryology • 4th-7th weeks gestation … the heart divides into 4 chambers via formation of swellings (cushions) of tissue that exhibit differential growth. • Endocardial cushions divide the AV canal forming the mitral and tricuspid valves. • Conotruncal cushions form the outflow tracts, aortic and pulmonary roots.
Embryology • 5th week gestation … the conotruncal cushions. • Right superior truncal cushion grows distally and left-ward. • Left inferior truncal cushion grows distally and right-ward. • The net effect is a twisting motion. • The truncal cushions fuse to form the truncal septum. • Additional cushions develop in the conus which grow down and towards each other until they fuse with the truncal septum to form the RVOT and LVOT.
Embryology • Mechanism of great artery transposition • Conotruncal cushion defect • Leads to failure of the conotruncal septum to spiral and instead extends straight downward • Aorta fuses with the RV and PA with the LV
Epidemiology • ~0.8% of live births are complicated by a cardiovascular malformation*. • >750,000 adult patients with congenital heart disease. • Transposition of the great arteries occurs in approximately 1 per 5,000 live births. • More common in males • Diagnosis possible in utero with fetal echocardiography • Transvaginal ultrasound at 13-14 weeks (limited views) • Transabdominal ultrasound at 16 weeks *not including bicuspid aortic valve and mitral valve prolapse
Complete transposition (D-TGA) • Pulmonary and systemic circulations are in parallel • Lethal, if no mixing (ASD, PDA, VSD) • ¾ are simple with no major associated abnormalities • ¼ are complex • VSD (16%) • Pulmonary/subpulmonary stenosis (9%) • Coarctation of the aorta (4%)
Complete transposition (D-TGA)Clinical Presentation and Outcomes • Larger size and weight at birth • Dyspnea and cyanosis • Progressive hypoxemia • Congestive heart failure • Without treatment, the outlook is dismal • 30% mortality within the 1st week • 90% mortality within the 1st year
Complete transposition (D-TGA)Management • Prostaglandin E1 to maintain the PDA • Atrial septostomy (balloon or surgical) • Palliative prior to corrective surgery • Repair within the first days to weeks of life • 2-4% mortality with 90% 1 year survival • Atrial switch • Mustard or Senning • Arterial switch • Rastelli procedure
Complete transposition (D-TGA) Atrial switch (Mustard/Senning) • Developed in the 1950s • Baffle directs venous return to contralateral ventricle
Complete transposition (D-TGA) Atrial switch (Mustard/Senning) • Disadvantages • RV functions as the systemic ventricle • Several significant long term complications • Congestive heart failure • Arrhythmias • Baffle leaks and obstruction • Pulmonary hypertension • Paradoxial embolus • Endocarditis • Overall survival 75% at 25 years • Senning may be better than Mustard [Moons et al, Heart 2004] • 340 patients (~⅔ Senning) compared • Less obstruction (1 vs. 15%) and better functional class with Senning • No significant mortality benefit
Complete transposition (D-TGA) Atrial switch (Mustard/Senning)Arrhythmias • Palpitations, presyncope, and syncope are not uncommon • Both brady and tachyarrythmias frequently seen • 50% develop sinus node dysfunction • Physical damage during surgery and baffle construction • Disruption of blood supply leading to ischemia • 20% develop atrial flutter • Sensitive to nodal agents due to conduction system disease • 11% required pacemakers at 20 years [Gelatt et al, J Am Coll Cardiol 1997] • Pacemakers are difficult to place due to distorted anatomy • Should be avoided if residual intracardiac communications due to risk of paradoxical embolus and stroke
Complete transposition (D-TGA) Atrial switch (Mustard/Senning)Congestive heart failure • Most adult patients develop congestive heart failure • By 20 years most are NYHA Class I or II • RV filling compromised due to defects in baffle construction • Baffle leaks (Mustard>Senning) • Left-to-right shunts with pulmonary hypertension (7%) • Risk of paradoxical embolus and stroke • Indications for intervention include >1.5:1 left-to-right shunt or any right-to-left shunt • Baffle obstruction (5-15%, Mustard>Senning) • SVC>IVC manifesting as SVC syndrome or hepatic congestion/cirrhosis • Often undetected due to collateral venous drainage (e.g. azygous vein) • 40% develop right ventricular dysfunction • 10-40% develop 2+ or greater tricuspid (systemic AV valve) regurgitation • Annular dilatation from RV failure • Damage from surgery or endocarditis
Complete transposition (D-TGA) Arterial switch • Developed in the 1980s • Great arteries and coronaries are transected and re-anastamosed
Complete transposition (D-TGA) Arterial switch • Advantages • LV is the systemic pump • No disruption of atrial conduction (sinus rhythm) • Fewer long term complications compared to atrial switch • Coronary ostial stenosis • Supravalvular pulmonary/aortic stenosis • Intervention indicated for RVOT gradient >50 mmHg • Neoaortic regurgitation • Arrhythmias • Follow up with normal LV function and good exercise capacity
Complete transposition (D-TGA) Rastelli procedure • TGA with VSD and LVOT obstruction • Outcomes • RV-PA conduit obstruction • Exercise intolerance/angina • RV failure • Intervention for RV-PA gradient >50 mmHg • LV-Ao patch obstruction • Dyspnea or syncope
Complete transposition (D-TGA) RV Failure after Atrial Switch • Standard heart failure therapies are unproven • The two-stage arterial switch • Stage 1 – the PA is banded to ‘re-train’ the LV to handle systemic pressures • Stage 2 – the atrial baffles and pulmonary band are taken down and an arterial switch is performed • 50% survival at 8 years in early results • Appears to be more successful in patients under 12
Congenitally corrected transposition (L-TGA) • A rare disorder that may present in adulthood. • Associated anomalies (95% of patients) • VSD (75%, commonly perimembranous) • Pulmonary stenosis (75%, commonly subvalvular) • Tricuspid valve anomalies (>75%) • Congenital complete heart block (5%)
Congenitally corrected transposition (L-TGA)Outcomes • Arrhythmias • Abnormal AV node and His positions • Dual AV nodes • 2% per year incidence of complete heart block • Susceptible to fibrosis of conduction system • Median survival 40 years • Mortality from progressive RV failure or arrhythmias • Tricuspid regurgitation is major predictor
Congenitally corrected transposition (L-TGA)Double Switch Procedure
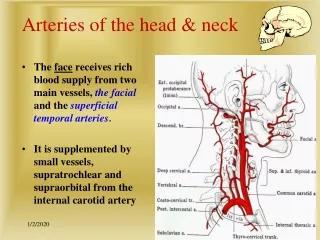
EchocardiographySegmental approach to congenital heart disease • Position of the apex • Situs of the atria • Morphological atria based on anatomic appearance of their appendages • 75% concordance with abdominal situs (aorta and IVC positions) • Atrioventricular relationship • Differentiate the morphological RV from LV: • Trabeculated apex • Moderator band • Septal attachment of the tricuspid valve • Lower (apical) insertion of the tricuspid valve • Ventriculoarterial relationship • Pulmonary artery is distinguished by its early branching pattern • Curved contour of the aortic arch with three major branches
EchocardiographyComplete Transposition with Atrial Switch • Hallmark is parallel great arteries (parasternal long axis) • Aorta is anterior to PA
EchocardiographyComplete Transposition with Atrial Switch • Systemic hypertrophied RV septum bows into LV • May impact TR and enhance subpulmonary stenosis
EchocardiographyComplete Transposition with Atrial Switch • Aortic and pulmonic valves lie in the same plane • Aorta is anterior and to the right (parasternal short axis)
EchocardiographyCongenitally Corrected Transposition • Hallmark is reversed offsetting of the AV valves • Aorta is anterior and to the left (parasternal short axis)
EchocardiographySpecial Considerations • Atrial switch • RV function • Tricuspid regurgitation • Subpulmonary obstruction • Baffle leak or obstruction (color Doppler) • Normal baffle flow is phasic with peak velocity <1 m/sec • Arterial switch • Neoaortic valve regurgitation • Supraneopulmonary valve stenosis • Wall motion abnormalities due to coronary artery ostial stenosis • Rastelli procedure • LV-Ao tunnel patch obstruction • RV-PA conduit degeneration (stenosis/regurgitation)
Endocarditis Prophylaxis ACC/AHA 2008 Guidelines state that antibiotic prophylaxis is reasonable to consider for patients at the highest risk of adverse outcomes (Class IIa) • Prosthetic valves • Prior endocarditis • Congenital heart disease • Unrepaired cyanotic, including palliative shunts and conduits • Completely repaired with prosthetic material or device (6 months) • Repaired with defects at or near a prosthetic device • Post-cardiac transplant with valvular disease
References • Webb et al., Congenital Heart Disease in Braunwald’s Heart Disease, 8th ed., Chapter 61, 1561-1624. • Sadler, Cardiovascular System in Langman’s Medical Embryology, 8th ed., Chapter 11, 208-259. • Otto, The Adult with Congenital Heart Disease in Clinical Echocardiography, 4th ed., Chapter 17, 418-447. • Warnes, Transposition of the Great Arteries, Circulation 2006 114:2699-2709. • Love et al., Evaluation and Management of the Adult Patient with Transposition of the Great Arteries Follow Atrial-level (Senning or Mustard) Repair, Nature Clinical Practice Cardiovasc Med 2008 5:454-67. • Verhuegt et al., Long-term Prognosis of Congenital Heart Defects: A Systematic Review, Int J Cardiol 2008 131:25-32. • Skinner et al., Transposition of the Great Arteries: from Fetus to Adult, Heart 2008 94:1227-35 • ACC/AHA Guidelines for the Management of Adults with Congenital Heart Disease, J Am Coll Cardiol 2008 52:e1-121.