Download
1 / 52
550 likes | 995 Views
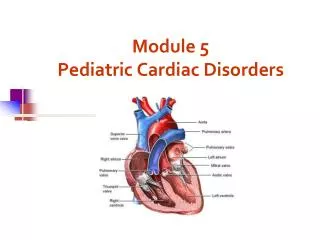
Module 5 – Pediatric Cardiac Disorders. Revised, Summer 2008. Fetal Circulation. Changes in Circulation. Umbilical cord clamped Pulmonary Pressure Pulmonary resistance. Critical thinking:. When are most cardiac anomalies discovered?

E N D
Module 5 – Pediatric Cardiac Disorders Revised, Summer 2008
Changes in Circulation • Umbilical cord clamped • Pulmonary • Pressure • Pulmonary resistance
Critical thinking: • When are most cardiac anomalies discovered? • What is included in the initial cardiac assessment of a newborn? • Why?
Assessment • History • Physical • Diagnostic
Importance of the Nurse Knowing Normal Value for O2 Saturations • Children respond to severe hypoxemia with BRADYCARDIA • Cardiac arrest in children generally r/t prolonged hypoxemia • Hypoxemia is r/t to respiratory failure or shock • BRADYCARDIA is a significant warning sign of cardiac arrest
Clinical Manifestations • Pump Fails – cannot meet the demands of the body = CHF How do you know when something is wrong? • Tires easily during feeding • Periorbital edema, weight gain • Rales and rhonchi • Dyspnea, orthopnea, tachypnea • Diaphoretic / sweating • Tachycardia • Weight
Goal of Treatment: • Improve cardiac function • Remove accumulated fluid and Na+ • Decrease cardiac demands • Decrease O2 consumption
Medications: • Digoxin –what do we assess prior to administration? • Which VS? Weigh diapers for strict I & O • Double check • Digoxin levels • Parent teaching • Digitalis toxicity • ACE inhibitors • Capoten (Captoril) • Vasotec
Medications continued… • Furosemide (Lasix) • Chlorothiazide (Diuril) • Zarozolyn (Thiazide type) • Spironolactone (Aldactone)
Nursing care • Reduce metabolic needs • Diet therapy • Decrease Cardiac Demands • Improve tissue oxygenation
Classifying congenital heart defects • By defects that increase pulmonary blood flow • Patent ductus arteriosus • Atrial septal defect • Ventricular septal defect • By defects that decrease blood flow and mixed defects • Pulmonic stenosis • Tetralogy of Fallot • Tricuspid atresia • Transposition of the great arteries • Truncus arteriosus
Signs & Symptoms What is most common indication of a congenital heart defect?
Cardiac catheterizations • Used to determine anomalies • Measures O2 sats in cardiac chambers and great arteries • Evaluates cardiac output • Identify detailed images of blood flow patterns • May allow for corrective or palliative measures
Nursing interventions pre and post cardiac catheterization • Assessment pre-op for baselines • Assessment post-op: • Vital signs (which ones are priority?) • Extremities • Activity • Hydration • Medications • Comfort measures
Teaching after cardiac catheterization • Parental teaching • Watch for s/s of bleeding, bruising at site • Foot temp on side of cath cooler • Loss of sensation in foot on side of cath • When to call the physician • If any of above s/s noted within 1st 24 hrs
Blood shunts from aorta (left) to the pulmonary artery (right) Returns to the lungs causing increase pressure in the lung Congestive heart failure Patent Ductus Arteriosus
Treatment • Medical Management • Medication • Indomethacin • Surgical • ____Ligate the ductus arteriosus
Nursing Care: • Pre-op • Patient/parent teaching • Assess for infection • Obtain lab values for chart • Post-op • ABCs • Rest • Hydration/nutrition • Prevent complications • Discharge teaching
Atrial Septal Defect • Oxygenated blood is shunted from left to right side of the heart via defect • A larger volume of blood than normal must be handled by the right side of the heart hypertrophy • Extra blood then passes through the pulmonary artery into the lungs, causing higher pressure than normal in the blood vessels in the lungs congestive heart failure
Treatment • Medical Management • Medications – digoxin • Surgical repair • Suture or simple patch
Treatment • Device Closure – Amplatzer septal occluder During cardiac catheterization the occluder is placed in the Defect
Ventricle Septal Defect • Oxygenated blood is shunted from left to right side of the heart via defect • A larger volume of blood than normal must be handled by the right side of the heart hypertrophy • Extra blood then passes through the pulmonary artery into the lungs, causing higher pressure than normal in the blood vessels in the lungs congestive heart failure
Treatment Surgical repair with a patch inserted
Pulmonic or Aortic Stenosis • Narrowing of entrance that decreases blood flow • Treatment: • Medications – Prostaglandins to keep the PDA open • Cardiac Catheterization • Balloon Valvuloplasty • Surgery • Valvotomy
Coarctation of the Aorta • Narrowing of Aorta causing obstruction of left ventricular blood flow • Left ventricular hypertrophy • Signs and Symptoms • B/P in upper extremities • B/P in lower extremities • Radial pulses full/bounding and femoral or popliteal pulses weak or absent • Leg pains, fatigue • Nose bleeds
Treatment • Goals of management are to improve ventricular function and restore blood flow to the lower body. • Medical management with Medication • A continuous intravenous medication, prostaglandin (PGE-1), is used to open the ductus arteriosus (and maintain it in an open state) allowing blood flow to areas beyond the coarctation. • Balloon dilation • Surgery Resect narrow area Anastomosis
Tetralogy of Fallot • 1. Four defects with right to left shunting • Signs and Symptoms • Failure to thrive • Lack of energy • Infections • Polycythemia • Clubbing of fingers • Squatting • Cerebral absess • Cardiomegaly • Cyanosis 2 1. 3 4
Treatment • Surgical interventions • Blalock – Taussig or Potts procedure – increases blood flow to the lungs. • Open heart surgery
Ask Yourself ? • Laboratory analysis on a child with Tetralogy of Fallot indicates a high RBC count. The polycythemia is a compensatory mechanism for: a. Tissue oxygen need b. Low iron level C. Low blood pressure d. Cardiomegaly
Mixed blood flow Survival depends upon mixing of blood from pulmonic and systemic circulation Cyanotic Disorders: • Truncus arteriosus • Hypoplastic left heart • Transposition of the great arteries
Truncus arteriosus • A single arterial trunk arises from both ventricles that supplies the systemic, pulmonary, and coronary circulations. A vsd and a single, defective, valve also exist. • Entire systemic circulation supplied from common trunk.
Hypoplastic heart • May have various left-sided defects, including coarctation of the aorta, aortic valve & mitral valve stenosis or artresia
Aorta arises from the right ventricle, and the pulmonary artery arises from the left ventricle – not compatible with survival unless there is a large defect present in ventricular or atrial septum. Transposition of Great Vessels aorta
Nursing Diagnosis & Goals: DX: Alteration in cardiac output: decrease R/T heart malformation Goal: Child will maintain adequate cardiac output AEB:
Nursing Care: • Monitor VS • I&O • Medications • Position • Metabolic rest • Assess and document child/family interactions • Parent teaching
Kawasaki Disease Mucocutaneous lymph node syndrome • Not contagious • Preceded by upper respiratory tract infection • Cause unknown
Clinical Manifestations: • Acute Phase- 10-14 days • Subacute Phase 10-25 days • Convalescent Phase 25-60 days
Diagnosis: • ECG • CBC, WBC • PT • ESR • SGOT, SGPT • IgA, IgG and IgM
Nursing Care: • Medication Therapy • Aspirin • Gamma Globulin • Nursing Interventions • Assess/monitor • Decrease stimulation • Comfort measures • Discharge teaching
Rheumatic Fever • Systemic inflammatory disease • Follows group A beta-hemolytic streptococcus infection • Causes changes in the entire heart especially the valves
Clinical Manifestations • Jones Criteria • Major • Minor • Supporting Evidence
Therapeutic Intervention • Medication • long term • prophylaxis • Nursing • Prevention • Parent teaching (ANTIBIOTICS)
Subacute Bacterial Endocarditis Infectious disease involving abnormal cardiac tissue: • Usually rheumatic lesions or congenital defects • Infection may invade adjacent tissues- aortic and mitral valves
Clinical Manifestations: • Onset insidious • Fever • Lethargy/general malaise • Anorexia • Splenomegaly • Retinal hemorrhages • Heart murmur –90% • Diagnosis- positive blood cultures