Download
1 / 22
220 likes | 444 Views
Cardiac Muscle II. Excitation-contraction coupling in the heart. There are 3 key differences in excitation-contraction coupling in heart versus skeletal muscle.

E N D
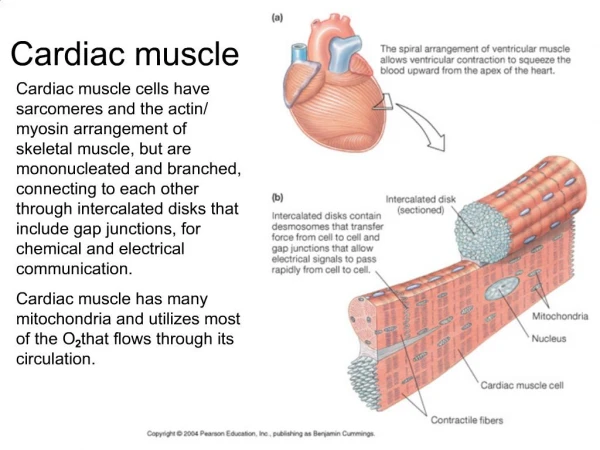
There are 3 key differences in excitation-contraction coupling in heart versus skeletal muscle • 1. In the myocardium, a significant amount of Ca++ (about 1/10 of the total) enters through L Ca++ channels in the sarcolemma, during the plateau of the myocardial action potential. • (In comparison, essentially all the Ca++ released in skeletal musclecomes from the SR and virtually none enters across the sarcolemma).
2. In the heart, the concentration of Ca++ attained in the sarcoplasm during an action potential is generally less-than-saturating for cardiac troponin. Therefore, unlike skeletal muscle, it is possible to modulate contractile force by modulating the amount of Ca++ that enters the sarcoplasm during excitation.
3. Ca++-induced Ca++ release is much more important in cardiac muscle than in skeletal muscle The Ca++ that enters through L channels both triggers, and tightly regulates, the amount of Ca++ released from the SR by ryanodine receptors in Ca++-induced Ca++ release. Each L channel in the sarcolemma controls a small number of nearby ryanodine receptors on the SR.
Opening of an L channel results in a small area of increased Ca++ that has been termed a “Ca++ spark” because it appears as a glowing spot when visualized with fluorescent Ca++ indicators. Trigger Ca++ Ca++ spark Ryanodine receptor Ca++ from SR
Regulation of myocardial performance • Two kinds: • Intrinsic: stretch increases force - the degree of stretch of the ventricle wall is determined by venous return - the amount of blood that enters the heart duringthe interbeat interval • Extrinsic: Cholinergic input decreases force; sympathetic input increases it. These inputs are managed by a reflex circuit that regulates arterial blood pressure.
Intrinsic regulation (autoregulation) • As averaged over several heartbeats, volume in = volume out • I.e. cardiac output = venous return • This is known as the Frank-Starling Law of the Heart
Some definitions: • End-diastolic volume EDV: the volume of the ventricle at the end of filling, equal to the venous return volume plus the end-systolic volume ESV. • Stroke volume SV: the amount of blood ejected during a beat. • SV = EDV-ESV
Cardiac Output is the volume of blood pumped by the heart per unit time = SV X HR Because of the Frank-Starling Law, the output of the two ventricles is equal, when averaged over time intervals of more than a few beats
The effect of the Frank-Starling Law on cardiac performance Venous return EDV Ventricular stretch Stroke Volume Since SV X HR = CO, CO follows VR
The Frank-Starling Law is the result of the position of the working heart on the rising limb of the length tension curve. For a time it was thought that the heart had parallel elastic elements that squeezed the sarcomeres, forcing them to greater overlap than in resting skeletal muscle.
However, recent studies showed that the slope of the length-tension curve of cardiac muscle is too steep to be explained simply as a result of the overlap of thick and thin filaments. Even more recent studies published in 2011 (Science 1333, 1440-1445) showed how stretch is transduced into an increase in Ca2+ release.
Single-cell studies of Starling’s law • In these studies, single cardiomyocytes were glued between two glass rods. One rod included a force transducer; the other could apply small increments of stretch. • The cells were loaded with a fluorescent Ca2+ probe.
In these figures you can see that stretching leads immediately to an increase in the number of Ca2+ sparks, represented as spikes on the false-color surface in figure B. In a real-life situation this would increase the baseline level of Ca2+ that would be present at the start of a heartbeat. The higher this baseline level is, the higher the peak level reached in an action potential, and thus the more crossbridges activated. This effect seems to be able to account for much if not all of the stretch-sensitivity of cardiac muscle.
Stretch causes regulatory subunits of membrane-associated NADPH oxidase (NOX2) to be brought in contact with its catalytic subunits. As a result, reactive oxygen species are released.
The stretch response is altered in genetic disease The results in the lower figure are from an animal model of Duchenne’s muscular dystrophy. In this case, stretch results in a wave of increased Ca2+ that could potentially trigger an arrhythmic heartbeat.
Effects of the beta adrenergic receptor in myocardium • Increased activity of L Ca++ channels • Increased sensitivity of troponin to Ca++ • Increased ability to clear Ca++ after a contraction – through reuptake to the SR and expulsion across the sarcolemma
What factors could increase the peak intracellular Ca++ concentration attained during excitation? • Simply increasing heart rate • Increased stretch during diastole • Activating Beta1 receptors • Cardiotonic drugs, such as digitalis, that interfere with Ca++ removal from the cytoplasm.
The effect of increased contractility on the length-tension relationship Increasing the inotropic state of the myocardium shifts the cardiac function curve upward and to the left. This means that the heart has become more sensitive to stretch.