Download
1 / 4
40 likes | 107 Views
No evidence to support the use of hydrochlorothiazide for 24-h blood pressure control. Objective: To asses the efficacy of hydrochlorothiazide on 24-h blood pressure (BP) control. Methods:

E N D
No evidence to support the use of hydrochlorothiazide for 24-h blood pressure control • Objective: • To asses the efficacy of hydrochlorothiazide on 24-h blood pressure (BP) control. • Methods: • Review of all the randomized trials that assessed 24-h BP with hydrochlorothiazide (HCTZ) compared with other antihypertensive drugs. • Meta-analysis of: • 14 studies of HCTZ dose 12.5 to 25 mg, • 5 studies of HCTZ dose 50 mg. 1. Messerli FH et al. J Am Coll Cardiol. 2011;57:590-600.
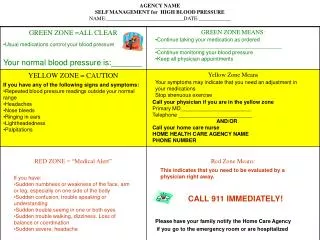
HCTZ: inferior 24-h BP control HCTZ ACE inhibitors ARBs Beta Blockers Calcium Antagonists 0 -5 N=14 BP Reduction (mm Hg) -10 N=3 -15 N=5 N=5 Systolic BP Diastolic BP N=7 -20 Efficacy of hydrochlorothiazide, assessed by 24-h ABPM1(Adapted fromMesserli FH et al. J Am Coll Cardiol. 2011;57:590-600) Compared with hydrochlorothiazide (HCTZ) dose 12.5 to 25 mg, P< 0.001 for other antihypertensive drugs, as assessed by 24-h ambulatory blood pressure (ABP) monitoring. Bars = 95% confidence intervals N = number of studies ACE = angiotensin-converting enzyme ARBs = angiotensin-receptor blockers 1. Messerli FH et al. J Am Coll Cardiol. 2011;57:590-600.
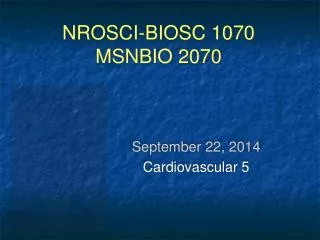
-39% -14% -43% Total mortality Fatal stroke Stroke -18% -30% Cardiovascular mortality Fatal or nonfatal stroke -21% -64% Renal events Heart failure -21% Total mortality “Not all diuretics are equal” HCTZ 12.5 - 25 mg/day does not reduce stroke and heart attack, or death.2,3 The diuretics shown to reduce cardiovascular morbidity and mortality are chlorthalidone in SHEP and ALLHAT, and indapamide in HYVET, PROGRESS, and ADVANCE 4 5 6 2. Gaciong Z, Symonides B. Expert Opin. Pharmacother. 2010;11:2579-2597.3. Kaplan NM. Hypertension. 2009;54:951-953. 4. Beckett NS, Peters R, Fletcher AE, et al. N Engl J Med. 2008;358:1887-1898. 5. PROGRESS Collaborative Group. Lancet. 2001;358:1033–1041. 6. ADVANCE Collaborative Group. Lancet. 2007;370:829-840.
CONCLUSIONS The efficacy on 24-h blood pressure control of HCTZ at its usual daily doses, of 12.5 to 25 mg/day is inferior to that of all other antihypertensive drug classes.1 There are no data showing that HCTZ 12.5 - 25 mg/day reduces heart attack and stroke or death.2 The authors of the meta-analysis concluded that: “if a clinical indication calls for a thiazide-type diuretic, chlorthalidone or indapamide remain the drugs of choice”.1 1. Messerli FH et al. J Am Coll Cardiol. 2011;57:590-600. 2. Gaciong Z, Symonides B. Expert Opin. Pharmacother. 2010;11:2579-2597.