Download
1 / 45
630 likes | 1.26k Views
Enterobacteriaceae. Meningitis. Opportunistic pathogens Escherichia coli Klebsiella pneumoniae Enterobacter aerogenes Serratia marcescens Proteus spp. Providencia spp. Citrobacter spp. Pneumonia. Sepsis. Diarrhea. UTI. Obligate pathogens Salmonella spp. Shigella spp.

E N D
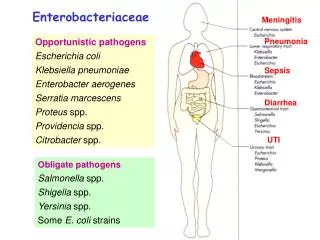
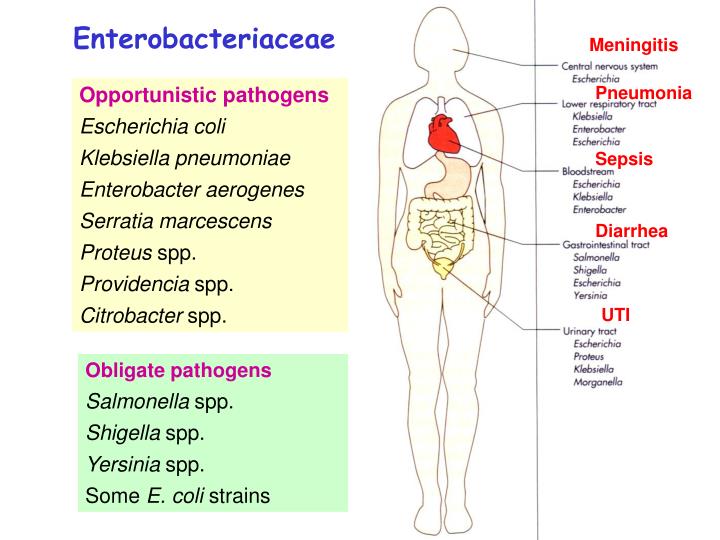
Enterobacteriaceae Meningitis Opportunistic pathogens Escherichia coli Klebsiella pneumoniae Enterobacter aerogenes Serratia marcescens Proteus spp. Providencia spp. Citrobacter spp. Pneumonia Sepsis Diarrhea UTI Obligate pathogens Salmonella spp. Shigella spp. Yersinia spp. Some E. coli strains
Morphology and Physiology Klebsiella spp. have large capsule (form large and very mucoid colonies); those of Enterobacter have smaller capsule; the others produce diffusible slime layers (form circular, convex and smooth colonies). Short gram-negative rods. Facultative anaerobes. Grow readily and rapidly on simple media. K. pneumoniae
Some enteric bacteria are motile. Klebsiella species are not motile, while Proteus species move very actively by means of peritrichous flagella, resulting in "swarming" on solid medium. Some strains of E. coli produce hemolysis on blood plates. Proteus spp.
Enterobacteriaceae is characterized biochemically by the ability to reduce nitrates to nitrites and to ferment glucose. Cytochrome oxidase-negative. Enterobacteriaceae species differ in their ability to ferment lactose. Some ferment lactose rapidly, some does it slowly and the others (e.g., Salmonella and Shigella) do not ferment lactose at all. Some Enterobacteriaceae pathogens (e.g., Salmonella and Shigella) are resistant to bile salts, and this property can be used to select them from commensal organisms that are inhibited by bile salts.
Antigenic Structure O antigens O-specific polysaccharides located in LPS. Heat-stable and resistant to alcohol. A single organism may carry several O antigens. (Core polysaccharide of LPS: enterobacterial common antigen) K antigens External to O antigens in some strains. Mostly are capsular antigens (polysaccharides). K antigens of Klebsiella can be identified by capsular swelling test. H antigen Flagellin. Heat-labile and denatured by alcohol. May be absent or undergo phase variation in different species.
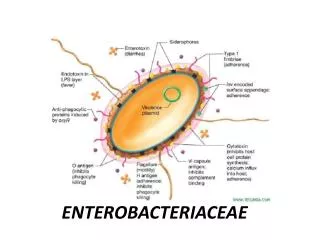
Pathogenesis and Immunity Common virulence factors Endotoxin (Lipid A of LPS) Capsule Antigenic phase variation Acquisition of growth factors (e.g. Fe) Resistance to serum killing Antimicrobial resistance Type III secretion systems: possessed by some Enterobacteriaceae pathogens, e.g., E. coli, Yersinia, Salmonella, and Shigella; facilitate transport of bacterial virulence factors directly into host cells.
Toll-like receptor 4 (TLR-4) Pathogenesis of sepsis caused by gram-negative bacteria
Pathophysiological effects of LPS Activation of complement, release of cytokines, fever, leukocytosis, thrombocytopenia, impaired organ perfusion and acidosis, disseminated intravascular coagulation (DIC), hypotension, shock and death, premature labor and abortion.
Escherichia coli Pathogenesis and clinical diseases Sepsis For people with inadequate host defenses, e.g. the newborns. Usually originates from UT or GI infections. Some infections may be endogenous. Meningitis E. coli (particularly K1 strains) and S. agalactiae are the leading causes of meningitis in infants. Bacteremia
Escherichia coli Pathogenesis and clinical diseases Urinary tract infection E. coli is the most common cause of urinary tract infection. Community- vs. hospital-acquired UT infection Most infections originate from colon; the bacteria contaminate the urethra, ascend into the bladder, and may migrate into the kidney or prostate. Symptoms: urinary frequency, dysuria, hematuria, and pyuria. Can result in bacteremia and sepsis. Uropathogenic E. coli strains produce P (Pyelonephritis-associated) pili, which is associated with renal colonization and may induce protective immunity, and hemolysin HlyA.
Escherichia coli Pathogenesis and clinical diseases EAST & PET Gastroenteritis (Diarrhea) Caused by various virotypes: Enterotoxigenic E. coli Enteropathogenic E. coli Enterohemorrhagic E. coli Enteroinvasive E. coli Enteroaggregative E. coli ST Table 30-2
Escherichia coli Pathogenesis and clinical diseases Enterotoxigenic E. coli(ETEC): major causal agent of Traveler's diarrhea. These strains express: a) Heat-labile (LT-1) enterotoxins: an A-B toxin. Subunit A causes intense and prolonged hyper secretion of chloride ions and inhibits the reabsorption of sodium and chloride. The gut lumen is distended with fluid, and hypermotility and secretory diarrhea occur, lasting for several days. It stimulates the production of neutralizing antibodies, and cross-reacts with the enterotoxin of Vibrio cholerae. b) Heat-stable (STa) enterotoxin: also stimulates fluid secretion; poorly immunogenic; short onset. c) Colonization factors (CFAs): facilitate the attachment of E. coli strains to intestinal epithelium. Usually are pili in nature.
ADP-ribosylation Enhance chloride secretion Decrease sodium and chloride absorption
Escherichia coli Pathogenesis and clinical diseases Enteropathogenic E. coli(EPEC):causes infant diarrhea in poor countries. Watery diarrhea results from malabsorption due to microvilli destruction. Spread by person-to-person contact. Enteroinvasive E. coli(EIEC):closely related to Shigella in pathogenic properties. Enteroaggregative E. coli(EAEC):causes chronic diarrhea and growth retardation in infants in developing countries.
Escherichia coli Pathogenesis and clinical diseases Enterohemorrhagic E. coli (EHEC) The most common strains producing disease in developed countries. These strains are associated with hemorrhagic colitis and hemolytic uremic syndrome (HUS: acute renal failure, microangiopathic hemolytic anemia and thrombocytopenia; 5-10% infected children). Serotpe O157:H7 is most commonly isolated. Cattle is a reservoir, and hamburger, unpasteurized milk, fruit juices, and uncooked vegetables are common sources of human infection. Induces A/E lesions on enterocytes. Diarrhea and HUS may be associated with the Shiga toxins, which are A-B toxins that bind to 28S rRNA and disrupt protein synthesis.
Other opportunistic Enterobacteriaceae Klebsiella K. pneumoniae and K. oxytoca are the most commonly isolated. Can cause community-acquired primary lobar pneumonia (frequently involves necrotic destruction of alveolar space), and infections of wound, soft tissue, and urinary tract. Risk factors for pneumonia: alcoholism; compromised pulmonary function. *In Taiwan: liver abscess is commonly seen in infection by K. pneumoniae. K. granulomatis may cuase granuloma inguinale, a sexually transmitted disease, in some countries. K. rhinoscleromatis: granulomatous disease of the nose. K. ozaenae: chronic atrophic rhinitis.
Proteus Most common isolates: P. mirabilis. Cause urinary tract infections and bacteremia. Produce urease, making the urine of the patients of UT infection with Proteus alkaline, promoting stone formation by precipitating Mg and Ca. Enterobacter, Citrobacter, Morganella, Serratia Opportunistic pathogens causing nosocomial infections in neonates and immunocompromised patients. These genera, particularly Enterobacter, are resistant to multiple antibiotics.
Escherichia coli and other opportunistic Enterobacteriaceae Laboratory diagnosis Smears: the Enterobacteriaceae pathogens resemble each other. The presence of large capsules is suggestive Klebsiella. Culture: blood agar and selective differential media (e.g., MacConkey agar), the latter is useful for preliminary identification. Commercial biochemical test systems can be used for identification of Enterobacteriaceae members. Serologic tests are used for determining the clinical significance of an isolate and for epidemiologic purpose.
E. coli and other opportunistic Enterobacteriaceae Treatment Variation in drug susceptibility is great, and antibiotic sensitivity tests are essential. Diarrhea patients usually need only symptomatic relief. Antibiotic treatment may prolong the fecal carriage or increase the risk of secondary complications. Treatment of bacteremia and septic shock: prompt antibiotic treatment, restoration of fluid and electrolyte balance, and treatment of disseminated IV coagulation.
E. coli and other opportunistic Enterobacteriaceae Prevention and control Enterobacteriaceae are a major part of normal flora and a common contaminant of the environment. In hospitals, opportunistic Enterobacteriaceae are commonly transmitted by personnel, instruments, or parenteral medications. Their control depends on hand washing, rigorous asepsis, sterilization of equipment, disinfection, restraint in IV therapy, and strict precautions in keeping the urinary tract sterile.
Salmonella Salmonella spp. do not ferment lactose. Most species of Salmonella are motile with peritrichous flagella. Some Salmonellae have capsular antigens; that of S. Typhi is referred to as Vi antigen. Groups and species of Salmonella are identified by serologic analysis of O and H antigens (> 2,500 serotypes). Classification of salmonellae is traditionally based on serogrouping and serotyping (e.g. S. typhimurium, which is reclassified as S. entericatogether with most human pathogens by analysis of DNA homology). The correct name for S. typhi is S. enterica, serovar. Typhi or S. Typhi. They can be identified by biochemical tests and serogrouping, with follow-up serotyping confirmation.
Salmonella Epidemiology S. Typhi and S. Paratyphi are primarily infective for humans. Other salmonellae are chiefly pathogenic in animals (poultry, pigs, rodents, cattle, pets etc.) that constitute thereservoir for human infection. Humans usually become infected by ingestion of contaminated food or drink (mean infective dose: 106-108, but that of S. typhi is lower). In children, infections can result from direct fecal-oral spread. The most common sources of human infections: poultry, eggs, dairy products, and foods prepared on contaminated work surfaces. However, the major source of infection for enteric fever is the carriers (convalescent or healthy permanent).
Salmonella Pathogenesis and Immunity Invasion Acid tolerance response (ATR) gene protects the organism from gastric acid. The bacteria invade into (by inducing membrane ruffling) and multiply in the M cells and enterocytes of the small intestine. They can also be transported across the enterocytes and released into the blood and lymphatic circulation. Inflammatory response confines the infection to the GI tract in non-typhoid salmonellosis. Survival in macrophages Salmonellae are facultative intracellular pathogen.
Salmonella Clinical diseases 1. Enteritis Incubation period: 6-48 hours. Symptoms: nausea, headache, vomiting, nonbloody profuse diarrhea, with few leukocytes in the stools. Low-grade fever, abdominal cramp, myalgia, and headache are also common. Episode resolves in 2-7 days. Inflammatory lesions of the small and large intestine are present. Stool cultures remain positive for several weeks after clinical recovery.
Salmonella Clinical diseases 2. Bacteremia Most common causal species: S. Choleraesuis, S Typhi and S. Paratyphi. Symptoms: like sepsis caused by other gram-negative bacteria. 10% of patients may have localized suppurative infections, e.g., osteomyelitis, endocarditis, arthritis, etc. High risk population: pediatric and geriatric patients; AIDS patients.
Salmonella Clinical diseases 3. Enteric fever (typhoid fever) Causal species: S. Typhi, S. Paratyphi A, S. Schottmuelleri, and S. Hirschfeldii. Mouth small intestine lymphatics and bloodstream infect liver, spleen and bone marrow multiply and pass into the blood second and heavier bacteremia onset of clinical illness colonization of gallbladder invasion of the intestine typhoid ulcers and severe illness. Chronic carriers (1%-5% of patients): bacteria persist in the gallbladder and the biliary tract for more than one year.
Symptoms: incubation time: 10-14 days. Gradually increasing fever, malaise, headache, myalgias, and anorexia, which persist for a week or longer. In severe cases: intestinal hemorrhage and perforation. Principal lesions: hyperplasia and necrosis of lymphoid tissue, hepatitis, focal necrosis of the liver, and inflammation of the gallbladder, periosteum, lungs and other organs.
Salmonella Treatment Enteric fever and bacteremia require antibiotic treatment: chloramphenicol, ampicillin, trimethoprim-sulfamethoxazole. Surgical drainage of metastatic abscesses may be required. Salmonella enterocolitis needs only supportive therapy (antibiotic treatment may prolong the symptoms and excretion of the salmonellae). Drugs to control hypermotility of the gut should be avoided because it is easy to transform a trivial gastroenteritis into a life-threatening bacteremia by paralyzing the bowel. Chronic carriers of S. Typhi may be cured by antibiotics alone or combined with cholecystectomy.
Salmonella Prevention and control Sanitary measures. Carriers must not be allowed to work as food handlers. Strict hygienic precautions for food handling. Vaccines against S. Typhi: Purified Vi antigen Oral, live attenuated vaccine.
National salmonella death toll rises to 7 (Staff writer Ridgely Ochs contributed to this story. January 24, 2009) A seventh death was linked Friday to a nationwide outbreak of salmonella associated with tainted peanut butter and paste sourced to the Peanut Corp. of America's plant in Blakely, Ga., authorities confirmed. Although their exact causes of death have not been determined, all seven people have died after being infected with the bacterial strain Salmonella Typhimurium, the Centers for Disease Control and Prevention said on its Web site. There have been 493 cases reported in 43 states and one Canadian province of people sickened, though authorities stress the numbers sickened are likely far in excess of that as many cases go unreported. Known patients ranged in age from 1 to 98, and 22 percent of the those have been hospitalized. Another 10 firms Friday recalled products that use PCA peanut butter or paste - bringing to roughly 360 the number of products affected - as it emerged that the Peanut Corp. of America's plant in Blakely, Ga. laid off most of its roughly 50 workers. The outbreak has triggered a congressional inquiry and renewed calls for reform of food safety laws. http://www.newsday.com/services/newspaper/printedition/saturday/health/ny-lisalm246010666jan24,0,5876138.story
Shigella S. dysenteriae, S. flexneri , S. sonnei , & S. boydii: bacillary dysentery > 45 O serotypes; have no H antigen; do not ferment lactose. Pathogenesis and Immunity Shigellosis is primarily a pediatric disease, and is restricted to the GI tract. Mean infective dose: 103. Mouth colon invade M cells and subsequently spread to mucosal epithelial cells cause microabscess in the wall of colonand terminal ileum necrosis of the mucous membrane, superficial ulceration, bleeding, and formation of pseudomembrane. Shiga toxin An A-B toxin inhibiting protein synthesis. Damages intestinal epithelium and glomerular endothelial cells (associated with HUS) .
Destablize the intestinal wall Activates the invasion genes on the virulence plasmid M cell Internalized shigellae induce apoptosis of macrophage and release of the bacteria Attracted by the cytokines released by macrophage
Shigella Clinical diseases Incubation period: 1-3 days Sudden onset of abdominal pain, fever and watery diarrhea number of stools increase, less liquid, often contain mucus and blood, rectal spasms with resulting lower abdominal pain (tenesmus) symptoms subside spontaneously in 2-5 days in adult cases, but loss of water and electrolytes frequently occur in children and the elderly a small number of patients remain chronic carriers. Some cases were accompanied by hemolytic uremic syndrome (HUS).
Shigella Laboratory diagnosis Specimens: fresh stool, mucus flecks, and rectal swabs. Large numbers of fecal leukocytes and some RBC may often be seen microscopically. Culture: differential and selective media as used for salmonellae. Treatment Antibiotic treatment: chloramphenicol, ampicillin, tetracycline, and trimethoprim-sulfamethoxazole. Drug resistance is common. Opiates should be avoided.
Shigella Prevention and control Humans are the only reservoir for shigellae. Transmission of shigellae: water, food, fingers, feces, and flies. Most cases occur in children under 10 years of age. Prevention and control of dysentery: 1. Sanitary control of water, food and milk; sewage disposal; and fly control. 2. Isolation of patients and disinfection of excreta. 3. Detection of subclinical cases and carriers.
Yersinia Y. pestis: plague ("black death") Y. pseudotuberculosis and Y. enterocolitica: gastroenteritis Grows more rapidly in media containing blood or tissue fluids and fastest at 30 oC. Some species (e.g. Y. enterocolitica) can grow in refrigerated food. Pathogenesis The Yersinia pathogens are able to resist phagocytic killing by secreting proteins into the phagocyte and result in inhibition of killing by phagocyte, apoptosis of macrophage, and suppression of cytokine production. Y. pestis produces a protein capsule (Fraction 1), and Pla (plasminogen activator protease) that degrades C3b and C5a, and fibrin clot (enhances spread of bacteria into blood stream).
Yersinia pestis Causes zoonotic infections; humans are accidental hosts. Three major pandemics have occurred in 541 AD, 1320s and 1860s. Two forms of infections: Urban plague Rats as natural reservoirs. Spread among rats or between rats and humans by infected flea. Can be eliminated by effective control of rats and better hygiene. Sylvatic plague: infections of rodents and domestic cats. Y. pestis are widely distributed in mammalian reservoirs and flea vectors and produces fatal infections in animal reservoirs. Human infections are acquired by contacting the reservoir population.
Yersinia pestis Pathogenesis Bubonic plague Y. pestis enters a flea when it feeds on an infected animal the bacteria multiply in the gut of the flea flea becomes hungry and bites ferociously Y. pestis passes from the flea into the bite wound the bacteria are phagocytised, but can multiply intracellularly or extracellularly reach the lymphatics, and an intense hemorrhagic inflammation develops in the enlarged lymph nodes, which may undergo necrosis Y. pestis may reach the bloodstream and become widely disseminated. Hemorrhagic and necrotic lesions may develop in all organs. Primary pneumonic plague Results from inhalation of infective droplets (usually from a coughing patient), with hemorrhagic consolidation of the lung, sepsis and death.
Yersinia pestis Clinical Diseases Bubonic plague Incubation period: 2-7 days. High fever and painful lymphoadenopathy with greatly enlarged, tender lymph nodes (buboes) in the groin and axilla sepsis (early stage: vomiting and diarrhea; late stage: hypotension, renal and cardiac failure; terminal stage: pneumonia and meningitis). Mortality: 75% if untreated. Pneumonic plague Incubation time: 2-3 days. Fever and malaise, pulmonary signs develop within 1 day. Patients are highly infectious. Mortality: 90% if untreated.
Yersinia pestis Treatment Patients have to be promptly treated with antibiotics (drug of choice: streptomycin). Epidemiology and control Plague is an infection of wild rodents that still occurs in many parts of the world (enzootic areas: India, Southeast Asia, Africa, and North and South America). Control of plague requires surveys of infected animals, vectors, and human contacts, and by destruction of infected animals. All patients with suspected plague should be isolated. Contacts of patients with suspected pneumonic plague should receive tetracycline as chemoprophylaxis.
Y. enterocolitica and Y. pseudotuberculosis Cause zoonotic infections. Y. enterocolitica is a common cause of enteritis in cold areas during the cold months. Y. pseudotuberculosis infection is relatively uncommon. They are found in the intestine of a variety of animals, and are transmissible to humans through contaminated food, drink or fomites, resulting in diarrhea, fever and abdominal pain that last for 1-2 weeks or, in some cases, months. Most are self-limited. Y. enterocolitica infection can cause pseudoappendicitis (enlarged mesenteric lymph nodes) in children, and blood-transfusion related sepsis in those who used blood products stored for at least 4 weeks.
Y. enterocolitica grows slowly at 37 oC and prefers cooler temperatures. The fecal specimen can be mixed with saline and then store at 4 oC for 2 weeks or more to facilitate isolation of this organism (cold enrichment).
Lipopolysaccharide (LPS) is also called endotoxin. LPS is composed of lipid A, core polysaccharide, and O-specific polysaccharide. Lipid Aanchors LPS in the lipid bilayer. It causes symptoms associated with endotoxin. O-specific polysaccharide can be used to identify certain species and strains. Back