Download
1 / 17
170 likes | 427 Views
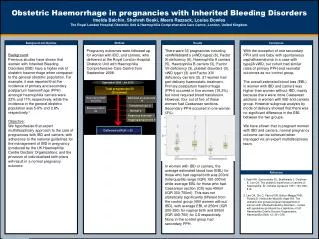
Obstetric Haemorrhage in a Resource-poor Setting. Max Brinsmead PhD FRANZCOG July 2010. Obstetric haemorrhage is. The major cause of maternal death in resource-poor countries The risk is increased by: Severe anaemia Other medical & obstetric conditions Poverty Transport problems

E N D
Obstetric Haemorrhage in a Resource-poor Setting Max Brinsmead PhD FRANZCOG July 2010
Obstetric haemorrhage is... • The major cause of maternal death in resource-poor countries • The risk is increased by: • Severe anaemia • Other medical & obstetric conditions • Poverty • Transport problems • Cultural & religious practices
Although the average gravida’s blood volume is expanded by 1.5L and all clotting factors are increased... • Blood loss of 10% or >500ml →Tachycardia • Loss of 25% or 1250ml→Vasoconstriction • Pale & cold extremities • Weak thready pulse • But systolic BP may be maintained • Loss of 33% or 2000ml →Hypotension • Sweating, pallor, thirst & oliguria • Greater blood loss → Risk of organ damage • Air hunger, restlessness & confusion • DIC and ARDS • >50% loss of blood volume → Cardiorespiratory arrest
Beware of the patient who survives large PPH elsewhere and arrives 24 – 48 hours later • May have a Hyperkinetic Circulation… • Rapid, full volume pulse • Normal BP • However JVP is raised and there are basal lung creps • This is anaemic Congestive Cardiac Failure… • And requires careful transfusion with IV Frusemide
After major obstetric haemorrhage the first priority is adequate IV access • 14G peripheral line • Use hot towels to vasodilate • Ideally one in each arm • Femoral vein puncture next best option • Jugular vein line with CVP is even better • Long saphenous cutdown next option • Femoral Artery catheterisation may be required • Pressure suit may be a first aid alternative
Jugular Vein Catheterisation • Position supine with 15 degree head-down tilt, head to the left • Skin asepsis, Lignocaine 1% • Identify the two heads of the sternomastoid muscle • Incise the skin at the apex of these muscles • The vein is deep to the clavicular head of this muscle and lateral to the carotid artery at the level of the cricoid cartilage • Use 16G cannula attached to 5 ml syringe • Advance subcutaneously at 30-degree angle towards the nipple • Aspirate until the vein is reached • Attach manometer which should oscillate with resps. • Complications: • Pneumothorax • Air embolism • Arterial puncture • Haematoma • Sepsis & thrombosis
Saphenous vein cut down • Position supine, leg restraint, tourniquet desirable • Skin asepsis, Lignocaine 1% • The vein is 2 cm above and 2 cm anterior to the medial malleolus • Incise the skin transversely • Identify the vein by dissection with fine arterial forceps, separate from adjacent nerve and strip clean for 2 cm • Place two loops of silk behind the vein • Tie off the distal end and loose tie the proximal • Open the vein with iris scissors or scalpel, using traction on the distal suture • Tourniquet release • Introduce a blunt plastic cannula, advance and allow blood to backflow, tighten the upper silk ligature • Suture secure and close the skin • Complications: • Infection • Delayed healing & keloid scar
It is desirable to... • Check that your cannula is in a vein before commencing infusion • Check by blood aspiration • X-ray for CVP placement • The zero mark of a CVP is aligned with the level of the R. atrium • 5 – 8 cm of H20 is normal • Begin infusion with Hartmanns • But only 700 ml of each litre remains intravascular • Albumin is the best colloid but Gel-fusion is a good substitute • Blood is best • May require delivery pressure • Fluid warming desirable
Your patient is stabilised when... • Systolic BP is > 100 mm AND • Pulse rate is < 100 / min • Put in a bladder catheter to monitor urine output • CVP is better, of course
Placenta Previa • After appropriate resuscitation delivery is indicated when… • The fetus is mature • The fetus is dead or severely malformed • Continuing haemorrhage threatens • The patient is unwilling or resources prevent continuing hospitalisation • Examination under anaethesia → Caesarean if… • The placenta is palpable through 2 or more fornices • The presenting part cannot be brought into the pelvic brim • During Caesarean Section… • Lower segment preferred • Consider ligation of major vessels • Go above the placenta to perform ARM & delivery • Use Green-Armytage to control bleeding after incision • A place for bipolar version and bringing down a leg • Requires > 4 cm dilation of the cervix • Attach a 1.5 Kg weight to the ankle • The buttock compresses the placenta • While the thigh dilates the cervix • Don’t attempt delivery until fully dilated
Placental Abruption • If the Uterus is > Dates or… • The fetus is dead then… • Assume major blood loss • As a guide to fluid replacement: • If the BP is 100 mm give 1,000 ml • If the BP is <80 mm give 2,000 ml • Plan delivery if >36 weeks • Examination under anaesthesia may be required • An early recourse to CS maybe life saving for the fetus • But do not begin CS until resuscitation is complete and coagulation has been checked • A rapid infusion of cryoprecipitate and platelets is desirable • Aim for vaginal delivery by amniotomy and oxytocin infusion when there has been fetal death • But monitor coagulation and • Prepare for PPH
Postpartum Haemorrhage • Begin aggressisve Rx earlier when there is… • Severe anaemia (HB <7.0) • Severe pre eclampsia • Prolonged labour • Principles: • Secure adequate IV access ASAP • Empty the uterus • Contract the uterus by oxytocics • Ergometrine, Syntocinon, Rectal Misoprostol • Bimanual uterine compression or • Aortic compression • Compress the bleeding site • Pack the vagina • Intrauterine balloon tamponade • Surgical options • Internal iliac artery ligation • B-Lynch suture • Hysterectomy • Uterine artery embolisation
Intrauterine Balloon Tamponade BJOG Review May 2009 Was effective in 91.5% of cases Combined retrospective and prospective studies But only a total of 106 patients Types of balloons Sengstaken Blakemore (GI use) Rusch (Urological) Foley (often multiple) Bakri (Specifically designed for obstetrics) Condom (+/- Foley) But there remain many unanswered questions
Questions concerning intrauterine balloon tamponade BJOG Review May 2009 Is it effective There are no RCTs Risks and contraindications Which balloon to use, how to insert it and what volume to inflate it Is a vaginal pack required Is an oxytocin infusion required Antibioitics and analgesia When to deflate and or remove it
When a patient presents with a retained placenta of >24 hours... • First resuscitate, transfuse and give antibiotics • Delay placental removal (for up to 48 hrs if required) • Prepare for morbid adherence of the placenta • During EUA after PPH always consider… • The possibility of uterine rupture • For secondary PPH up to 7 days after birth… • Uterine “curage” with 2 fingers is safer • For secondary PPH more than 7 days after birth… • Suction is safer than traditional curette • And remember to give antibiotics for sufficient time before EUA to control generalised sepsis
Renal Failure after Obstetric Haemorrhage • Diagnosis… • Less than 400 ml urine in 24 hours • Beware of toxicity from any drugs usually excreted by the kidneys • Avoid fluid and sodium overload during the oliguric phase • Strict fluid balance • Mannitol or Frusemide • Bicarbonate infusion for acidosis • Ion exchange resin or dialysis for hyperkalaemia • Avoid dehydration in the diuretic phase • Strict fluid balance • May require up to 10 litres/day