Download
1 / 2
20 likes | 160 Views
Development of a detuned oral assay for recent HIV infection. F. Priddy 1 , P. Phelan 1 , P. Tambe 1,2 , C. del Rio 1. MoPe15.2C26. 1 Emory University School of Medicine, 2 Fulton County Department of Health and Wellness. 603 Church Street Decatur, GA 30030, USA; fpriddy@emory.edu. Abstract

E N D
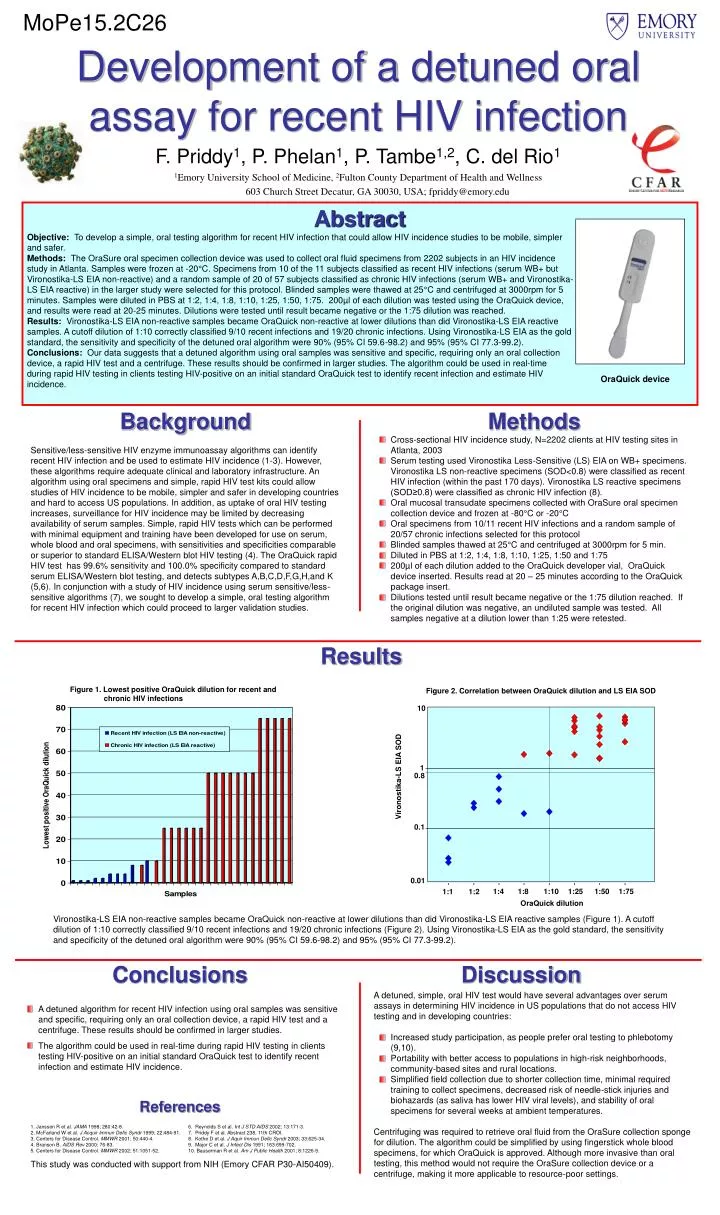
Development of a detuned oral assay for recent HIV infection F. Priddy1, P. Phelan1, P. Tambe1,2, C. del Rio1 MoPe15.2C26 1Emory University School of Medicine, 2Fulton County Department of Health and Wellness 603 Church Street Decatur, GA 30030, USA; fpriddy@emory.edu Abstract Objective: To develop a simple, oral testing algorithm for recent HIV infection that could allow HIV incidence studies to be mobile, simpler and safer. Methods: The OraSure oral specimen collection device was used to collect oral fluid specimens from 2202 subjects in an HIV incidence study in Atlanta. Samples were frozen at -20°C. Specimens from 10 of the 11 subjects classified as recent HIV infections (serum WB+ but Vironostika-LS EIA non-reactive) and a random sample of 20 of 57 subjects classified as chronic HIV infections (serum WB+ and Vironostika-LS EIA reactive) in the larger study were selected for this protocol. Blinded samples were thawed at 25°C and centrifuged at 3000rpm for 5 minutes. Samples were diluted in PBS at 1:2, 1:4, 1:8, 1:10, 1:25, 1:50, 1:75. 200µl of each dilution was tested using the OraQuick device, and results were read at 20-25 minutes. Dilutions were tested until result became negative or the 1:75 dilution was reached. Results: Vironostika-LS EIA non-reactive samples became OraQuick non-reactive at lower dilutions than did Vironostika-LS EIA reactive samples. A cutoff dilution of 1:10 correctly classified 9/10 recent infections and 19/20 chronic infections. Using Vironostika-LS EIA as the gold standard, the sensitivity and specificity of the detuned oral algorithm were 90% (95% CI 59.6-98.2) and 95% (95% CI 77.3-99.2). Conclusions: Our data suggests that a detuned algorithm using oral samples was sensitive and specific, requiring only an oral collection device, a rapid HIV test and a centrifuge. These results should be confirmed in larger studies. The algorithm could be used in real-time during rapid HIV testing in clients testing HIV-positive on an initial standard OraQuick test to identify recent infection and estimate HIV incidence. OraQuick device Background Sensitive/less-sensitive HIV enzyme immunoassay algorithms can identify recent HIV infection and be used to estimate HIV incidence (1-3). However, these algorithms require adequate clinical and laboratory infrastructure. An algorithm using oral specimens and simple, rapid HIV test kits could allow studies of HIV incidence to be mobile, simpler and safer in developing countries and hard to access US populations. In addition, as uptake of oral HIV testing increases, surveillance for HIV incidence may be limited by decreasing availability of serum samples. Simple, rapid HIV tests which can be performed with minimal equipment and training have been developed for use on serum, whole blood and oral specimens, with sensitivities and specificities comparable or superior to standard ELISA/Western blot HIV testing (4). The OraQuick rapid HIV test has 99.6% sensitivity and 100.0% specificity compared to standard serum ELISA/Western blot testing, and detects subtypes A,B,C,D,F,G,H,and K (5,6). In conjunction with a study of HIV incidence using serum sensitive/less-sensitive algorithms (7), we sought to develop a simple, oral testing algorithm for recent HIV infection which could proceed to larger validation studies. Methods • Cross-sectional HIV incidence study, N=2202 clients at HIV testing sites in Atlanta, 2003 • Serum testing used Vironostika Less-Sensitive (LS) EIA on WB+ specimens. Vironostika LS non-reactive specimens (SOD<0.8) were classified as recent HIV infection (within the past 170 days). Vironostika LS reactive specimens (SOD≥0.8) were classified as chronic HIV infection (8). • Oral mucosal transudate specimens collected with OraSure oral specimen collection device and frozen at -80°C or -20°C • Oral specimens from 10/11 recent HIV infections and a random sample of 20/57 chronic infections selected for this protocol • Blinded samples thawed at 25°C and centrifuged at 3000rpm for 5 min. • Diluted in PBS at 1:2, 1:4, 1:8, 1:10, 1:25, 1:50 and 1:75 • 200µl of each dilution added to the OraQuick developer vial, OraQuick device inserted. Results read at 20 – 25 minutes according to the OraQuick package insert. • Dilutions tested until result became negative or the 1:75 dilution reached. If the original dilution was negative, an undiluted sample was tested. All samples negative at a dilution lower than 1:25 were retested. Results Figure 1. Lowest positive OraQuick dilution for recent and chronic HIV infections Figure 2. Correlation between OraQuick dilution and LS EIA SOD 10 1 0.8 Vironostika-LS EIA SOD 0.1 0.01 1:4 1:8 1:10 1:25 1:50 1:75 1:1 1:2 OraQuick dilution Vironostika-LS EIA non-reactive samples became OraQuick non-reactive at lower dilutions than did Vironostika-LS EIA reactive samples (Figure 1). A cutoff dilution of 1:10 correctly classified 9/10 recent infections and 19/20 chronic infections (Figure 2). Using Vironostika-LS EIA as the gold standard, the sensitivity and specificity of the detuned oral algorithm were 90% (95% CI 59.6-98.2) and 95% (95% CI 77.3-99.2). Conclusions Discussion A detuned, simple, oral HIV test would have several advantages over serum assays in determining HIV incidence in US populations that do not access HIV testing and in developing countries: • Increased study participation, as people prefer oral testing to phlebotomy (9,10). • Portability with better access to populations in high-risk neighborhoods, community-based sites and rural locations. • Simplified field collection due to shorter collection time, minimal required training to collect specimens, decreased risk of needle-stick injuries and biohazards (as saliva has lower HIV viral levels), and stability of oral specimens for several weeks at ambient temperatures. Centrifuging was required to retrieve oral fluid from the OraSure collection sponge for dilution. The algorithm could be simplified by using fingerstick whole blood specimens, for which OraQuick is approved. Although more invasive than oral testing, this method would not require the OraSure collection device or a centrifuge, making it more applicable to resource-poor settings. • A detuned algorithm for recent HIV infection using oral samples was sensitive and specific, requiring only an oral collection device, a rapid HIV test and a centrifuge. These results should be confirmed in larger studies. • The algorithm could be used in real-time during rapid HIV testing in clients testing HIV-positive on an initial standard OraQuick test to identify recent infection and estimate HIV incidence. References 1. Janssen R et al. JAMA 1998; 280:42-8. 6. Reynolds S et al. Int J STD AIDS 2002; 13:171-3. 2. McFarland W et al. J Acquir Immun Defic Syndr 1999; 22:484-91. 7. Priddy F et al. Abstract 238, 11th CROI. 3. Centers for Disease Control. MMWR 2001; 50:440-4. 8. Kothe D et al. J Aquir Immun Defic Syndr 2003; 33:625-34. 4. Branson B. AIDS Rev 2000; 76-83. 9. Major C et al. J Infect Dis 1991; 163:699-702. 5. Centers for Disease Control. MMWR 2002; 51:1051-52. 10. Bauserman R et al. Am J Public Health 2001; 8:1226-9. This study was conducted with support from NIH (Emory CFAR P30-AI50409).