Download
1 / 42
420 likes | 530 Views
Sleep Medicine Something Old / Something New. Glenn W. Burris, MD, MS, FAASM Medical Director The SOMC Sleep Diagnostic Center Portsmouth, Ohio. Learning Objectives.

E N D
Sleep MedicineSomething Old / Something New Glenn W. Burris, MD, MS, FAASM Medical Director The SOMC Sleep Diagnostic Center Portsmouth, Ohio
Learning Objectives • The learner will understand the basic components of a diagnostic polysomnogram and the speaker will explain the definitions of respiratory events used to calculate the Apnea-Hypopnea Index. • The speaker will present clinical guidelines for the use of unattended portable monitors in the diagnosis of obstructive sleep apnea • The learner will understand some of the health benefits of treating obstructive sleep apnea with nasal CPAP.
The Study of Sleep 1834 – Robert McNish “ Sleep is the intermediate state between wakefulness and death, wakefulness being regarded as the active state of all the animal and intellectual functions, and death as that of their total suspension.”
The Study of Sleep 1937 – Davis, Loomis, Harvey, Hobart - different stages of sleep were reflected in changes of the EEG 1953 – Asereinsky & Kleitman -Identification of Rapid Eye Movements during Sleep 1957 – Dement & Kleitman - Relationship between eye movements, body motility, and dreaming 1968 – Rechtschaffen and Kales (R&K) - standard sleep scoring technique 2007 – American Academy of Sleep Medicine - Manual for the Scoring of Sleep and Associated Events
Polysomnogram Continuous monitoring of physiology during sleep • Electroencephalogram (EEG) • Eye Movements • Nasal and Oral Air flow • Submental Muscle activity (EMG) • Respiratory Effort – Chest and Abdomen • Cardiac Rhythm • Leg Muscle Activity – tibialis anterior • Pulse oximetry • Snore Microphone • Video Monitoring
Polysomnogram Information is included in 30 second epochs
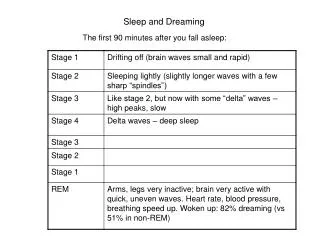
Polysomnogram Following completion of the study the information is scored: • Lights out • Sleep Latency – from lights out to onset of sleep • Sleep Stages • Non-REM – N1, N2, N3 • REM • Sleep Efficiency – percentage of time asleep • Respiratory Events • Leg Movements • Arousals • Heart Rhythms • Snoring intensity • Lights on • Quality of patient’s sleep compared to baseline
Scoring Respiratory Events Apnea – when all of the following criteria are met • There is a drop in the peak thermal sensor excursion by >90% of baseline • The duration of the event lasts at least 10 seconds • At least 90% of the event’s duration meets the amplitude criteria for apnea • Classified as: obstructive, central, or mixed based on respiratory effort Hypopnea – when all of the following are met 1) The nasal pressure signal excursion drops by 30% of baseline • The duration of this drop occurs for a period of at least 10 seconds • There is a 4% desaturation from pre-event baseline • At least 90% of the event’s duration meets the amplitude criteria The AASM Manual for the Scoring of Sleep and Associated Events, 2007
Obstructive Sleep Apnea Respiratory Disturbance Index (RDI) – no longer used • apneas, hypopneas, respiratory related arousals Apnea-Hypopnea Index (AHI) • total number of respiratory events / hours of sleep Severity of OSA defined by theAHI: less than 5 – not sleep apnea 5 – less than 15 – MILD 15 – less than 30 – MODERATE > 30 – SEVERE
Portable Monitoring for OSA in Adults In home diagnostic test for OSA Advantages • Convenience • Less costly • Attending technologist not required Disadvantage • Fewer physiologic variables that lead to misdiagnosis • Technical limitations (apparatus malfunction) = repeat studies • Validation of the device
Portable Monitoring for OSA in Adults Types of Monitoring Devices Type 1 – in sleep center, attended, overnight polysomnogram Type 2 – record same variables as type 1, unattended Type 3 – evaluate four physiologic parameters – not sleep respiratory movement and airflow heart rate arterial oxygen saturations (snoring), (position) Type 4 – evaluate one or two parameters (saturation and airflow)
Portable Monitoring for OSA in Adults Limitations of Type 3 devices • Apnea Hypopnea Index – abnormal breathing events by recording time as sleep can not be recorded • Unless the patient was sleeping the entire recording time, the AHI calculated by a portable monitor will likely be lower than an attended polysomnogram • Can not distinguish sleep stages
Portable Monitors and OSA 2005 Center for Medicare and Medicaid Services (CMS) • evidence was not adequate to conclude, tests remained uncovered 2008 • Reconsidered and will allow for coverage of CPAP therapy based on a positive diagnosis of OSA by home sleep testing • Must fulfill all requirements in the National Coverage Determination, CR6048 • Clinical evaluation as a positive diagnosis from PSG or unattended, type 2, 3, 4(measuring at least 3 channels) • Diagnostic tests that are not ordered by the beneficiary’s treating physician and not considered reasonable and necessary
Portable Monitors and OSA Clinical Guidelines for the Use of Unattended Portable Monitors in the Diagnosis of Obstructive Sleep Apnea in Adults Portable Monitoring Task Force of the American Academy of Sleep Medicine1 Clinical Guidelines for the Evaluation, Management, and Long-term Care of Obstructive Sleep Apnea in Adults2 1. J Clinical Sleep Medicine, Vol 3, 2007 2. J Clinical Sleep Medicine, Vol 5, 2009
Portable Monitors and OSA American Academy of Sleep Medicine Guidelines • Should be performed only in conjunction with a comprehensive sleep evaluation, preferably by a sleep medicine specialist • May be used as an alternative to PSG for the diagnosis of OSA in patients with a high pretest probability of moderate to severe OSA • Should not be used in patients who have comorbid medical conditions that predispose to sleep related breathing disorders • Must record air flow, respiratory effort and blood oxygen information
Portable Monitors and OSA Guidelines – cont • Experienced persons should educate the patient or directly apply the the monitoring equipment • Should be a method to monitor the quality of the recordings • Monitors must be capable of displaying the raw date for clinical review • All patients should have a follow-up visit with a provider able to discuss the results of the test
Obstructive Sleep Apnea Charles Dickens ( 1812 – 1870) The Posthumous Papers of the Pickwick Club • Described Joe, a fat boy, who was always excessively sleepy. A loud snorer. • First reported in 1965 during the study of severely obese patients 1 1. Brain Res 1965; 2: 167-186
Obstructive Sleep Apnea Wisconsin Sleep Cohort Study Random, n=602, ages 30 – 60 Sleep disordered breathing as high as: 24% of men 9% of women 4% of men, 2% of women had symptomatic OSA AHI - >5 Daytime hypersomnolence NEJM 1993;328(17):1230-35.
Risk of OSA in the US Population Results from the National Sleep Foundation Sleep In America 2005 Poll • n= = 1506 adults (775 were women) • Mean age 49 • Berlin Questionnaire • 26% of respondents (31% of men and 21% women) found to be at high risk of OSA As many as one in four American adults could benefit from an evaluation for OSA! CHEST 2006; 130: 780-786
Identifying Patients with OSA Clinical Presentation • Threshold to symptoms highly variable • Insidious • Unaware or underestimate their degree of impairment • Elderly patients aware of frequent awakenings • Complaints of insomnia and unrefreshing sleep • Excessive body movement, kicking in sleep • Decrements in short-term memory • Moodiness, irritability
Identifying Patients with OSA Clinical Presentation – cont • Lack of concentration • Anxiety / depression • Morning headaches – up to 50% • Sensation of choking / dyspnea • Decreased libido and impotence • GERD, worse at night • Nocturia, 28% of patients report 4 to 7 episodes of nightly
Obstructive Sleep Apnea “My wife made me come!”
Cardiovascular disease Hypertension Coronary Artery Disease Stroke Arrhythmia Pulmonary Hypertension Congestive Heart Failure Hematological Platelet Activation Hypercoaguable state Neurological TIA Stroke Daytime Fatigue Memory / Intellectual impairment Morning Headaches Gastrointestinal GERD Fatty Liver Metabolic Altered Leptin Levels Poor Gylcemic Control Rapid Weight Gain Psychological Depression Irritability / Mood Changes Nocturnal Panic Attacks Bed partner Relationships Genitourinary Impotence Nocturia Renal Proteinuria Focal Segmental Glomerulosclerosis Immune Elevated TNF-a Decreased IgM Elevated IL-6 Decreased NK cells Increased C3 Inflammation C-reactive protein Obstructive Sleep Apnea
Berlin Questionnaire A means of identifying patients with sleep apnea • n = 744 adults completed the questionnaire • 279 were in a high-risk group • 100 patients (equal representation of high and low risk group) underwent a portable sleep study • Being in the high-risk group predicted an RDI of greater than 5 with a sensitivity of 0.86 and a specificity of 0.77 Ann Intern Med, 1999, 131: 485-491
Obstructive Sleep Apnea Physical exam of the Upper Airway Lack of consensus in describing the physical findings Nose • Nasal Obstruction Oropharynx • Mallampati Class Retrognathia • Risk of narrow airway at the base of the tongue
Mallampati Class Scoring is as follows: Class 1: Full visibility of tonsils, uvula and soft palateClass 2: Visibility of hard and soft palate, upper portion of tonsils and uvulaClass 3: Soft and hard palate and base of the uvula are visibleClass 4: Only Hard Palate visible Can Anaesth Soc J, 1985 Jul; 32(4) 250-1
Mallampati Class Mallampati Score as an Independent Predictor of Obstructive Sleep Apnea n=137 80 (58%) had OSA as defined as AHI 5 or greater Likelihood Ratio Class I - 4 of 12 patients 0.4 Class II - 24 of 50 patients 0.7 Class III - 45 of 65 patients 1.6 Class IV - 7 of 10 patients 1.7 For every increase in Mallampati Score by one, • increased odds of having OSA by about 2 fold • the AHI increased by more than 9 events / hour Sleep 2006; 29 (7) 903-908
Obstructive Sleep Apnea - Hypertension Sleep Heart Health Study Multicenter Study, n= 6132 Age > 40 years, 53% female AHIHypertension <1.5 43% 1.5 – 4 53% 5 -14 59% 15 – 29 62% >30 67%JAMA 2000;283:1829-1836 JNC 7 – OSA identifiable cause of hypertension JAMA 2003; 289: 2560-2572
Obstructive Sleep Apnea - Hypertension Treatment of OSA with CPAP can Improve Hypertension 17 hypertensive patients, 7 normotensive patients Moderate to severe OSA (AHI 60 +/- 19) Four to six months CPAP NEJM 2000: 343:967
Obstructive Sleep Apnea – Congestive Heart Failure OSA in Dilated Cardiomyopathy: The effects of CPAP N = 8 Dilated cardiomyopathy and severe OSA (AHI 54) BaselineCPAP Left ventricle ejection fraction 37% 49% Stopped CPAP for one week 53% 45% Lancet 1991; 338:1480-4
Obstructive Sleep Apnea – Cardiac Remodeling Effects of Continuous Positive Airway Pressure on Cardiac Remodeling as Assessed by Cardiac Biomarkers, Echocardiography, and Cardiac MRI • Prospective Study, n = 52, years 2007-2010 • AHI > 15, Epworth Sleepiness Score >10 • Evaluation before CPAP, 3 mos, 6 mos and 12 mos • At each visit: TnT, CRP, and NT-proBNP levels, and a standard TTE • CMR at baseline and 6 and12 months after the initiation of CPAP treatment. CHEST 2012; 141(3):674–681
Obstructive Sleep Apnea - Cardiac Remodeling • Following 12 months of CPAP therapy, levels of CRP, NT-proBNP, and TnT did not change • As early as 3 months after initiation of CPAP, TTE revealed an improvement in right ventricular end-diastolic diameter, left atrial volume index, right atrial volume index, and degree of pulmonary hypertension, which continued to improve over 1 year of follow-up. • Left ventricular mass, as determined by CMR, decreased from 159 g/m 2 to 141 8 g/m 2 as early as 6 months into CPAP therapy and continued to improve until completion of the study at 1 year. CHEST 2012; 141(3):674–681
Obstructive Sleep Apnea - Diabetes CPAP Therapy of Obstructive Sleep Apnea in Type 2 Diabetics Improves Glycemic Control During Sleep • n=20, type 2 diabetes and newly diagnosed OSA • measured glucose levels every five minutes during sleep • baseline and after treatment with CPAP (average 41 nights) • Mean glucose decreased in 10 of 11 subjects with glucose > 100mg/dL • No decrease in subjects with glucose < 100mg/dL J of Clin. Sleep Med. Dec 15, 2008
Obstructive Sleep Apnea - Diabetes Impact of Untreated Obstructive Sleep Apnea on Glucose Control in Type 2 Diabetes • n = 60, 14 without OSA, 46 with OSA • Controlled for: sex, race, BMI, waist circumference, Hgb A1C, year of diagnosis, medications (insulin and oral), exercise, hypertension and snoring. • Increasing severity of OSA was associated with poorer glucose control. Am J RespirCrit Care Med Vol 181. pp 507–513, 2010
Obstructive Sleep Apnea - Diabetes Compared to controls the mean HbA1c: • Mild OSA - increased by 1.49% (P= 0.0028) • Moderate OSA - increased by 1.93% (P= 0.0033) • Severe OSA – increased by 3.69% (P< 0.0001) • Linear Trend (P< 0.0001) • inverse relationship between OSA severity and glucose control in patients with type 2 diabetes Am J RespirCrit Care Med Vol 181. pp 507–513, 2010
Obstructive Sleep Apnea – Mortality One of the first reports of adverse consequences was published 1988 8 year study, n=385 severe OSA compared to less severe OSA (AHI >20, <20) significant increase in all cause mortality (death) change in mortality corrected by tracheostomy and CPAP CHEST 1988; 94:9-14
Obstructive Sleep Apnea - Mortality Sleep Apnea as an Independent Risk Factor for All-Cause Mortality: The Busselton Health Study Sleep Apnea diagnosed Screened 380: 18 had moderate to severe OSA 77 had mild OSA followed up to 14 years 6 of the 18 died 33% (moderate to severe OSA) 5 of the 77 died 6% (mild OSA) SLEEP 2008 Vol 31, No 8
Obstructive Sleep Apnea – Mortality Sleep Disordered Breathing and Mortality: Eighteen-Year Follow-up of the Wisconsin Sleep Cohort n= 1546, mean observation period of 13.8 years AHI n Deaths 0 < 5 1157 46 (4%) 5 - <15 220 16 (7.3%) 15 - <30 82 6 (7.0%) >30 63 12 (19.75%) Cardiovascular death – 42% of persons with severe OSA 26% of persons without OSA SLEEP 2008 Vol 31, No 8
Clinical Pearls • Obstructive Sleep Apnea is a common medical condition that contributes significantly to a multitude of comorbid diseases • Presenting symptoms are heterogeneous and clinical evaluation should be frequently considered • Untreated OSA in intimately related to worsening of many medical conditions • Identification and treatment of OSA has a positive impact on individual health and health care resources