Download
1 / 66
680 likes | 1.3k Views
SR presentation Facial dysmorphic features. Alcohol and its associated skin manifestations. Christophe Francois HSU Moderator: Dr Joyce LEE Prepared under the guidance of Dr NG SK. History. 21 yo Chinese male Polytechnic student (no neurological impairement)

E N D
SR presentationFacial dysmorphic features.Alcohol and its associated skin manifestations Christophe Francois HSU Moderator: Dr Joyce LEE Prepared under the guidance of Dr NG SK
History • 21 yo Chinese male • Polytechnic student (no neurological impairement) • Was seen by urologists for operation for phimosis and referred for sclerodermiform features. • Complains of dry skin • PMH: operation for small eyes (cosmetic purposes), no problems on parturition, no developemental defect. No history of cardiac disease. • Family history: Mother has Sjogren’s syndrome, no siblings. No mention of alcohol exposure during pregnancy.
Clinical examination • Skin hardened to normal upon palpation. No surface changes • Palpebral fissure • Nose normal • No flattened groove between nose and upper lip • Small bilateral slit eyes • Microstomia • Low set ears • Ichthyosis on legs • Dentition normal • No genital anomalies
Differential Diagnosis • Fetal Alcohol Syndrome • Scleroderma • Syndromes with overlapping features with FAS: • Aarskog Syndrome • Williams Syndrome • Noonan’s syndrome • Cornelia de Lange Syndrome • Fetal hydrantoin (dilantin or phenytoin) syndrome • BPES type II
Investigations • Investigations • FBC, SCL-70 antibodies and ANA normal • No features of scleroderma upon biopsy
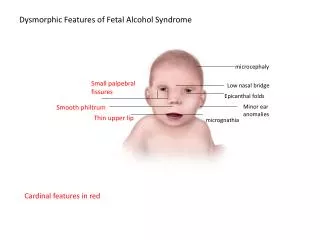
Fetal alcohol syndrome • Adverse neonatal and pediatric effects occur with maternal alcohol consumption during pregnancy. The diagnosis of fetal alcohol syndrome (FAS) is based on findings in the following 3 areas: -(1) characteristic facial anomalies -(2) growth retardation (intrauterine growth restriction and failure to have catch-up growth) (graded from none to severe (3rd percentile; 4-digit diagnostic code) -(3) CNS involvement (cognitive impairment, learning disabilities, or behavioral abnormalities).
FAS with/out confirmed maternal alcohol exposure • Partial FAS with confirmed maternal alcohol exposure • Other categories that can be used when heavy maternal alcohol use is documented and other causes are ruled out • Alcohol-related neurodevelopmental disorder (ARND) • Alcohol-related birth defects (ARBD)
Key characteristic craniofacial abnormalities • Smooth philtrum • Thin, smooth vermilion border of the upper lip • Low nasal bridge, small nose • Short palpebral fissures (<10th percentile for age) (small eye opening) • Skin folds at corner of the eye • Other craniofacial abnormalities • Midface hypoplasia • Microphthalmia • Strabismus • Ptosis • Small cranial perimeter (below 10th precentile)
Ranking FAS facial features is complicated because the three separate facial features can be affected independantly by prenatal alcohol: -Severe: -lip ranked 4-5 -philtrum ranked 4-5 -PFL ranked at 3 (one to 2 SD below average developed by the university of Washington) -Moderate: -2 features ranked as severe and one as moderate -Mild -2 facial features ranked severe and one within normal limits -One feature ranked severe and 2 moderate -1 severe, 1 moderate, one normal -None
Central nervous damage: -definite: structural (microcephaly, cerebellar hypoplasia, agenesis of corpus callosum) or neurologica impareiments(epilepsy, motor skills, deafness, coordination...) or static encephalopathy -probable: significant dysfunction of two or more sd in 3 or more functional domains -possible: one or 2 functional domains or clinical judgement it cannot be dismissed. -unlikely: no evidence
Prenatal alcohol exposure: • High risk: more than 100mg/dl in early pregnancy • Some risk: less than 100mg/dl or unknown usage patterns. • Unknown risk: adopted or adult patients, children in foster care. Stigmatizing also for mothers. • No risk: Confirmed absence of exposure which rules out the diagnosis
Causes • The risk of alcohol-related effects increases according to maternal consumption in a dose-dependent fashion. Furthermore, heavy episodic, or binge, drinking is the riskiest pattern of consumption. • Therefore, women who have the potential to become pregnant and who are binge drinkers may continue this pattern of consumption in the early weeks of an unrecognized pregnancy and therefore be at risk for FAS or FASD. • Evidence indicates that alcohol primarily affects brain development. Therefore, drinking in all 3 trimesters poses a risk.
Syndromes with overlapping features with FASAlcohol exposure is not present • Aarskog Scott Syndrome: • X linked-recessive. Mutation in FGDY1 in band p11.21 of X chromosome. • Short stature, facial anomalies (hypertelorism and downslanting palèpebral fissures, anteverted nostrils), genital anomalies (shawl scrotum: scrotum surrounding penis), skeletal anomalies, mental retardation
Williams Syndrome • Deletion of 26 genes on the long arm of chromosome 7 (q11.23) • Elfin facial appearance and low nasal bridge • Behavioural anomalies: cheerful bahaviour and ease with strangers, predisposition to violent outbursts. Also lack of common sense and impaired intelligence. Love for music. • -supravalvular aortic stenosis
Noonan’s syndrome (Male Turner’s): • Autosomal dominant, 12q24.1 mutation of PTPN11 which codes for a tyrosine phosphatase. • Facial features: triangular facies, small upturned nose, palpebral ptosis, hypertelorism, deeply grooved philtrum, keloids • ! Low set ears, backward rotated ears, Thick helix of ears • Learning problems • Congential heart malformation
Cornelia de Lange Syndrome • Autosomal dominant, mutation often spontaneous of NIPBL gene (2 others discovered since) • Clinical features • Microcephlia • Developmental delay • Facial features: long eyelashes, bushed eyebrows, synophrys (fused eyebrows), short upturned nose and thin downturned lips, long philtrum, low set ears
Fetal dilantin syndrome • one third of mothers taking this drug during pregnancy develop minor face and limb birth defects. • Features: low set deformed ears, midfacial hypoplasia, blepharoptosis and mild hypertelorism, short nose with a broad depressed bridge. Cleft palate • Small proportion have developmental delay, or mental retardation
LAST MINUTE! BPES Type II • Blepharophimosis, ptosis, epicanthus inversus syndrome. • Type II refers to just the eye changes without primary ovarian syndrome. • Type I, the mother will be infertile • Autosomal Dominant • The gene affected is Fox L2
So alcohol related birth defects? • Syndrome? • What other effects can alcohol have?
Table I. Dermatologic manifestations of alcohol use • and abuse • Specific dermatologic manifestations • Vascular • Spider telangiectasia • Palmar erythema • Corkscrew scleral vessels • Caput medusae • Plethoric facies • Flushing • Unilateral nevoid telangiectasia • Jaundice • Pruritus • Urticaria • Nail changes • Terry’s nails • Red lunulae • Koilonychia • Clubbing • Hyperpigmentation • Skin cancer • Lichenoid dermatitis • Oral changes • Black hairy tongue • Glossitis • Leukoplakia • Parotid swelling • Alcohol-induced diseases/disease states with associated • dermatologic manifestations • Nutritional deficiencies • Marasmus • Kwashiorkor • Pellagra • Scurvy • Endocrine diseases • Hypogonadism • Hyperestrogenism • Pseudo-Cushing’s syndrome • Porphyria cutanea tarda • Infections • Vibrio vulnificus sepsis • Acquired purpura fulminans • Pancreatitis • Subcutaneous fat necrosis • Cullen/Grey Turner’s sign • Dupuytren’s contracture • Madelung’s disease • Coagulopathy • Exacerbations of skin disease • Psoriasis • Rosacea • Discoid eczema
Table I. Dermatologic manifestations of alcohol use • and abuse • Specific dermatologic manifestations • Vascular • Spider telangiectasia • Palmar erythema • Corkscrew scleral vessels • Caput medusae • Plethoric facies • Flushing • Unilateral nevoid telangiectasia • Jaundice • Pruritus • Urticaria • Nail changes • Terry’s nails • Red lunulae • Koilonychia • Clubbing • Hyperpigmentation • Skin cancer • Lichenoid dermatitis • Oral changes • Black hairy tongue • Glossitis • Leukoplakia • Parotid swelling • Alcohol-induced diseases/disease states with associated • dermatologic manifestations • Nutritional deficiencies • Marasmus • Kwashiorkor • Pellagra • Scurvy • Endocrine diseases • Hypogonadism • Hyperestrogenism • Pseudo-Cushing’s syndrome • Porphyria cutanea tarda • Infections • Vibrio vulnificus sepsis • Acquired purpura fulminans • Pancreatitis • Subcutaneous fat necrosis • Cullen/Grey Turner’s sign • Dupuytren’s contracture • Madelung’s disease • Coagulopathy • Exacerbations of skin disease • Psoriasis • Rosacea • Discoid eczema Long list
Alcohol induced changes • Due to organ dysfunction (digestive tract) • Liver • Porphyria Cutanea Tarda • Cirrhosis • Pruritus • Jaundice • Pancreas • Pancreatitis
Alcohol induced changes • Generalized • Acute changes • Urticaria • Chronic changes • Skin Aging • Neoplasia • Malnutrition
Porphyria Cutanea Tarda (PCT) All porphrias are hereditary except PCT type I PCT type I also as symptomatic protoporphria -Epidemiology: affects males from 40 onwards, often with a history of alcohol abuse -Three categories -PCT I: symptomatic protoporphyria, non hereditary, 80% of PCTs, deficit in uroporphrinogen decarboxylase (only in hepatocytes) -PCT II: : autosomal dominant, less than 20% of PCTs), the deficit in uroporphyrinogen decarboxylase is also present in red blood cells. -PCT III: similar to PCTI in the sense that uroporphrinogen decarboxylase is only present in the hepatocyte (less than 5% of PCTs), but hereditary -Clinically -skin hyperfragility -serous-hemorrhagic bullae and erosions on dorsum of hands following minimal trauma -actinic bullosis: light-coloured bullae appearing after sun exposition. Then erosions form leaving scars with milia. -hypertrichosis: mostly in malar area -chronic actinic dermatosis: premature aging of the skin=diffuse brownish pigmentation, losangeal skin on the nape of the neck (nuchae rhomboidalis), diffuse elastoma and elastosis with cysts, comedones on the face. -in 1/3 of cases, scleroderma-like lesions appear lately on the face, neck, torso, trunk and scalp (scarring alopecia beginning from the hairline). In the preauricular area, these lesions calcify (microliths) and the ulcers they create only heal after they disappear.
Porphyria Cutanea Tarda (PCT) All porphrias are hereditary except PCT type I PCT type I also as symptomatic protoporphria -Epidemiology: affects males from 40 onwards, often with a history of alcohol abuse -Three categories -PCT I: symptomatic protoporphyria, non hereditary, 80% of PCTs, deficit in uroporphrinogen decarboxylase (only in hepatocytes) -PCT II: : autosomal dominant, less than 20% of PCTs), the deficit in uroporphyrinogen decarboxylase is also present in red blood cells. -PCT III: similar to PCTI in the sense that uroporphrinogen decarboxylase is only present in the hepatocyte (less than 5% of PCTs), but hereditary -Even in the hereditary types, alcohol among others has a trigger role. -Clinically -skin hyperfragility -serous-hemorrhagic bullae and erosions on dorsum of hands following minimal trauma -actinic bullosis: light-coloured bullae appearing after sun exposition. Then erosions form leaving scars with milia. -hypertrichosis: mostly in malar area -chronic actinic dermatosis: premature aging of the skin=diffuse brownish pigmentation, losangeal skin on the nape of the neck (nuchae rhomboidalis), diffuse elastoma and elastosis with cysts, comedones on the face. -in 1/3 of cases, scleroderma-like lesions appear lately on the face, neck, torso, trunk and scalp (scarring alopecia beginning from the hairline). In the preauricular area, these lesions calcify (microliths) and the ulcers they create only heal after they disappear. -extracutaneously, chronic hepatitis, cirrhosis, hepatocellular carcinoma. Even in the hereditary types, alcohol has a trigger role
Pruritus -It may appear up to 2 years before the onset of cirrhosis -40% of alcohol abusers with liver disease are estimated to have severe pruritus -generalized but with predilection to extensor extremities, upper trunk, palms and soles, -chemical mediators (Bile acids) are thought to directly depolarize nerve endings or release pruritogenes (histamine). -Treatment with bile acid-binding resins (cholestyramine) relieves the pruritus in 80% of cases, but malabsorption of ADEK. Also methyltestosterone or norethandrolone, UVA and UVB photoherapy. Phenobarbital (3mg/KG), intravenous albumin, extracorporeal photophoresis, diets rich in polyunsaturated acids. -Poor correlation with bile-levels/pruritus though.
Jaundice -due to the deposition of billirubin, product of the breakdown of heme: accumulation in the liver due to impaired hepatic conjugation. It subsequently binds tissues with a special affinity to elastin. -detectable with serum levels above 2,5 mg/dL -The ocular sclera are often the first to turn yellow. -DD prehepatic, hepatic, posthepatic -Rx abstinence resolves jaundice provided there is residual hepatic function.
Cirrhosis • Spider naevi: -present in 75% of the time -on the face and trunk -rarely unilateral of the naevoid type, which abundance would correlate with the existence of oesophageal varicosities (Foutch et al),
Nails • total apparent leuconychia (Terry’s nails): 80% of patients with cirrhosis. Proximal 2/3 white, presumed to result from reduced blood flow due to overgrowth of connective tissue.