Download
1 / 44
440 likes | 553 Views
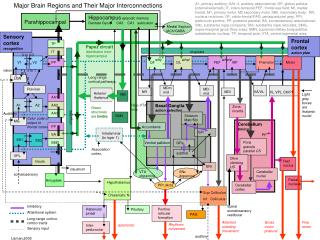
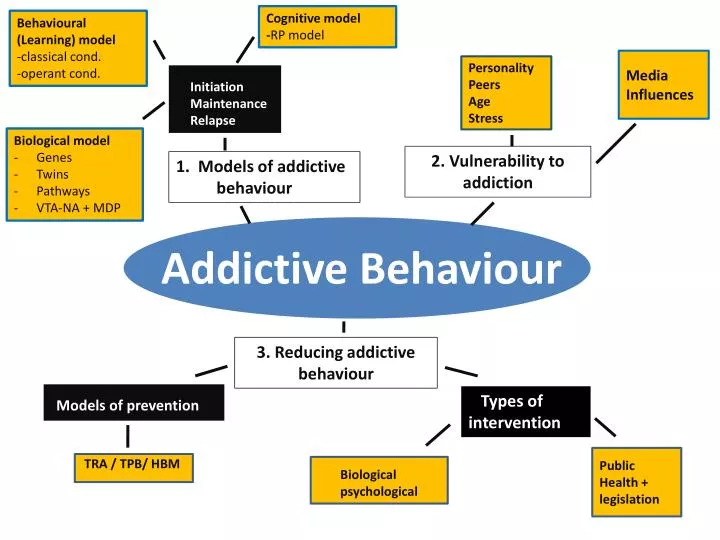
Cognitive model - RP model. Behavioural (Learning) model -classical cond. -operant cond. Media Influences. Personality Peers Age Stress. Initiation Maintenance Relapse. Biological model Genes Twins Pathways VTA-NA + MDP. 2. Vulnerability to addiction .

E N D
Cognitive model -RP model Behavioural (Learning) model -classical cond. -operant cond. Media Influences Personality Peers Age Stress Initiation Maintenance Relapse • Biological model • Genes • Twins • Pathways • VTA-NA + MDP 2. Vulnerability to addiction 1. Models of addictive behaviour Addictive Behaviour 3. Reducing addictive behaviour Models of prevention Types of intervention Public Health + legislation TRA / TPB/ HBM Biological psychological
Vulnerability to addiction • Risk factors in the development of addiction • Personality peers age stress • Media Influences
Addictive “Gateway” • Although the following explanations are set out by each factor (i.e. personality, peers, age, stress) you will find that there are some underlying ‘themes’ or reasons for people’s vulnerability to addictive behaviours, that are found in some/all of them. One example of this is the idea of a “gateway”. This refers to the idea that once you start an addictive behaviour you can be introduced to others by either; the same shared setting, your friends or perhaps the shared enjoyment and therefore these can lead to other addictive behaviours.
Group Activity – Prezi!!Risk factors in the development of addiction 1. Stress – e.g. Traumatic stress 2. Age/ Peers – e.g. SLT 3. Personality – addictive personality neuroticism/psychoticism 4. Mobile phone addiction - research
Could there be such a thing as .. … An ADDICTIVE PERSONALITY?? WHAT DO YOU THINK?
Personality ADDICTIVE PERSONALITY • There is a well-defined link between smoking/gambling addiction and a variety of anxiety disorders. • Personality profiles for individuals with high N (Neuroticism) – i.e. moodiness, irritability and anxiety, together with high levels of P (Psychoticism) – i.e. aggressiveness, emotional coldness , impulsivity – suggest an “addictive personality” (Eysenck and Eysenck (1985). • These characteristics are suggested to make these people more vulnerable to addiction. • The idea of an addictive personality is supported by the fact that certain individuals can become dependent on many things, either simultaneously or over time. For example, a gambling addict overcomes their dependency and then subsequently becomes addicted to alcohol (in taking its place).
Sample Questionnaire Try this Introverted-Extraverted Neuroticism-Psychoticism excerpt 1. Are you a rather lively person? ____ 2. Does your mood often change up and down without real reasons? ____ 3. Do you have many different hobbies? ____ 4. Are you a talkative person? ____ 5. Would you feel worried by making debt? ____ 6. Do you ever feel "just miserable" for no reason? ____ 7. Do you lock your door carefully for the night? ____ 8. Do you stop for a split of a moment thinking things over before doing anything? 9. Would you become upset to see a child or an animal suffer ? ____ 10. Do you often worry about things you should not have said or done ____ 11. Can you usually let yourself go and enjoy yourself at a lively party? ____ 12. Are you an irritable person? ____ 13. Do you like meeting new people? ____ 14. Do you believe insurance planning is a good idea ? ____ 15. Are your feelings easily hurt? ____ Total : score 1 = for each no score 5 for each yes
High score low score
Personality Research • Chein et al (1964) found that low self-esteem, negative outlook and learned incompetence characterised ghetto adolescent addicts, suggesting that individuals with personalities tending toward a negative outlook on life (i.e. pessimistic) are more vulnerable to addiction.
Limson et al (1991) compared alcoholics and non-alcoholics on levels of personality and assessed the relationship between personality and neurological mechanisms, by recording measures of cerebrospinal fluid concentrations. • Results showed that alcoholics had significantly different personality profiles and a negative correlation was found between aggression and levels of cerebrospinal fluid. This indicates some support for the idea that addiction is related to personality, which in turn is regulated by underlying neurobiology.
Activity – Use your A2 textbooks to answer the following (page 417) • Stretch and Challenge • Is there an “Addictive Personality”? In other words - are there individual traits/characteristics that make it highly likely that a person with those traits will develop some addictive behaviour THREE traits that make one individual more likely to develop some addictive behaviour than someone else. 1. Mood alteration (up today, down tomorrow) 2 Negative emotions (e.g feelings of failure) 3 Low self efficacy (don’t feel as important as others) Think: Is there a difference between those who experiment and those who abuse?
Peers • Peer pressure – is very influential and can affect an individual’s behaviour, especially during adolescence where peer groupings are a prime influence on attitudes and behaviour. If peer groupings have positive attitudes towards addictive behaviours, e.g. thrill seeking, experimentation, etc. then individuals within such peer groupings will have an increased vulnerability to dependency, indeed many individuals with addiction problems often blame the initiation and maintenance of their dependency on peer pressure.
Adherence to peer pressure can be seen as a form of conformity involving normative social influence, where individuals are influenced by peer pressure due to a desire to be accepted and avoid ridicule and rejection (Gross, 2012). • When a peer group adopts addictive behaviours as part of their ‘norms of behaviour’, then such behaviours can quickly become part of an individual’s ‘in-group repertoire’, used not only to show allegiance to the group, but also to identify the group as separate from other ‘out-groups’, that is, ones without positive attitudes to dependency behaviours.
Peer pressure can also be seen as a form of operant conditioning, where the group reinforces participation in and positive attitudes towards – addictive behaviours, by rewards of praise and increased status within the group. Peers also act as a form of social learning, modelling addictive behaviours so that other individuals will observe and imitate such behaviours, as a form of vicarious reinforcement (where behaviour is imitated to gain rewards seen as occurring to those modelling the behaviour).
Relapse • Peers can also be seen as influencing recovering addicts to relapse. Many addicts, after treatment, often return to their old social influences, including peer groups, where pressure may be experienced to return to dependency behaviours.
Research • Sussman and Ames (2001) found that friend and peer smoking is a strong predictor of smoking among teenagers, with deviant peer groupings role-modelling and offering cigarettes, demonstrating the influence of social networks in determining levels of individual vulnerability. • Wagner & Anthony (2002) found that smokers were more likely to progress to cocaine usage, due to being in peer groupings where there are opportunities for new drug experiences, showing how peers can act as a social context ‘gateway’ to other dependencies. • Leshner (1998) believed treatment strategies for smokers should include social context elements, such as peer groups, as well as biological and behavioural ones if they are to be successful, as recovered addicts may relapse when leaving a smoking clinic, due to the original social context still being in place.
AGE • The prime time for initiation of dependency behaviours, such as smoking, is during adolescence and there is a positive correlation between early onset of dependency behaviours and reduced probability of abstaining. 17.3 % of adolescents from 132 countries were classed as smokers in 2006. • Those who commence their addictions early are also more likely to relapse when trying to quit. Early onset of dependency behaviour is also related to increased likelihood of other dependency behaviours and as such early onset behaviours can be regarded as ‘gateway behaviours’ paving the way to other dependencies.
Although early experience of addictive substances and behaviours is highly correlated with later dependency, failure to quit and relapses after quitting, there is also an increased vulnerability in old age to addiction. • About a third of alcoholics develop their dependency after retirement, which suggests the change in lifestyle and/or status may be linked to this phenomenon, although another possible reason is the increased stresses of older age, such as boredom, and the death of loved ones. • Tranquilliser and sleeping tablet abuse have also been found to be problematic among elderly females.
Age Research • Shram (2008) measured age differences in neural responses to acute nicotine administration and to the rewarding and aversive effects of nicotine in adolescent and adult rats, self administering nicotine intravenously. Nicotine was found to have a greater activating effect on the neural structures of adolescents, who were also more sensitive to the rewarding qualities of nicotine, but less sensitive to it’s aversive effects. • Adults were more resistant to extinction and showed more aversive effects to nicotine withdrawal. The results, therefore, suggest that the rewarding effects of nicotine are highest in adolescence, demonstrating why this is a prime time for initiation of smoking, but also why quitting is more difficult for older adults.
HCYSS (Health Canada Youth Smoking Survey) (2006) compared smokers who started between 12-15 years of age, with non-smokers and found that early onset smokers were more likely to drink alcohol (91% compared to 52%), binge drink, (58% -23%) and smoke cannabis (50% - 5%). This implies that adolescent cigarette smoking is a ‘gateway’ (i.e. facilitating progression to other legal/illegal drug use.
Helfer (2006) found that 17% of Swiss women over 75 years of age use painkillers or sleeping tablets everyday and 6% also take tranquillisers. A huge increase in painkiller and tranquilliser usage was also noted between those of 55-64 years of age. As for alcohol, 46% of men over 75 drank every day, compared to 6% of 25-34 year olds. This suggests that the older a person is, the more likely they are to use certain addictive substances. • Research indicates that public health initiatives would be more effective if targeted at specific age groups • Dependency in old age is a sensitive area of research with older people reluctant to admit to, or talk about, their addictions. This has implications for treatment, as younger people may feel more able to admit to dependency problems and therefore seek help.
STRESS • Stress has for a long time has been seen as increasing vulnerability to addiction. The basic idea is that increased stress levels are positively correlated with an increased vulnerability to developing dependency habits, often as a maladaptive way of dealing with stress. • Such stressors can include things like neighbourhood disorganisation, poor housing and economic deprivation. It may be that certain individuals are more negatively affected by everyday stressors, which others find easier to cope with and therefore it may be that those who are more easily stressed - are more vulnerable to addiction.
Clip • Stress clip
The increased stresses, both biological and psychological, experienced when attempting to quit dependency behaviours and maintain quitting behaviour, may also be responsible for individuals relapsing back into dependency. • There is some evidence of molecular and cellular changes associated with chronic stress and addiction, drawn from brain-imaging studies and research into stress, cravings and their relationship to specific brain areas associated with reward and addiction risk.
Stress Research • Piazza et al (1989) investigated how stress affected vulnerability to addiction in rats, by demonstrating how previous repeated exposure to stressful tail-pinching and amphetamines increased activity in the dopamine neural system through behavioural sensitisation, making the rats more disposed to self-administer amphetamines. This suggests that stress affects drug taking via the action of neurobiology.
Kostenet al (2000) found that new born rats who were subjected to isolation stress for 1 hour a day on their 2nd to 9th days of life had a greater tendency to cocaine administration when adults, than rats who did not suffer isolation stress when new born. Although this affect was specific to cocaine, the results have important implications for the role of early childhood stress in vulnerability to addiction.
Cleck & Blendy (2008) reported that people with stress-related psychiatric disorders such as depression and anxiety, are often involved with addictive drug usage and exposure to chronic stressful life events, such as sexual abuse - are linked to increases in nicotine, alcohol and cocaine usage. • Also they suggest that the greater and longer an individual endures childhood abuse-is positively correlated with an increased likelihood of developing dependencies in later life. Stress exposure is also related to increases in current drug use and precipitates relapse back into dependency. • The findings strongly suggest a leading role for stress in determining vulnerability levels to addiction
Gross (2008) suggest that as much evidence of neurobiological changes associated with stress and addiction is correlational and as such does not indicate causality. Such neurobiological changes could just as easily be effects of stress and addiction than causes.
Also… ethics • ….much research into stress involves studying animals. This presents an issue of ‘extrapolation’ to humans. Studies done on animals due to the perception that such research would be unethical to perform on humans- is often justified by a cost-benefit analysis,where the benefit of the knowledge gained is seen to outweigh the harm caused to the animals. However, increasingly more people challenge this assumption and perceive such studies as inherently unethical. benefit cost
Timed essay “ Outline and discuss research into individual differences in vulnerability to addiction ” (8 + 16 marks)
Plan See VLE “model answer” • Describe one factor • Introduce debate/issue (Animal research) • Evaluate number one • Describe number two • Evaluate it • Don’t forget research method terms..