Download
1 / 31
370 likes | 705 Views
Tidal breathing analysis Reliability and Clinical Relevance of Tidal Breathing Analysis. H.J. Smith Product Manager Pneumonology Respiratory Care Turkish Thoracic Society 2014. Workshop tidal breathing analysis. Forced spirometry Education and training in all levels on all issues

E N D
Tidal breathing analysisReliability and Clinical Relevance of Tidal Breathing Analysis H.J. Smith Product Manager Pneumonology Respiratory Care Turkish Thoracic Society 2014
Workshop tidal breathing analysis Forced spirometry • Education and training in all levels on all issues • European spirometry driving licence • Everlasting problems • Quality of spirometry and test results will ever depend on efforts of patients and medical stuff • Interpretation of flow limitation needs expertise of physician Tidal breathing analysis • Little offers for specific training or education • Knowledge and skills are very often out-of-date • Misunderstanding in methodological potential, quality issues, relevance of test results • Promoted mostly by paediatricians Why not in combination with spirometry?
Introduction “Pro” tidal breathing analysis Tidal breathing lung function testing • Physiologic • Usual way of breathing • Effort independent (all subjects can be measured – from infants to elderly and severe diseased) • Maximal manoeuvres are limited in describing tidal breathing conditions • Of interest in diagnostics of the lung • Differentiated, informative, sensitive • Direct measurements of specific characteristics of the respiratory system
Spirometry tidal breathing analysis Mostly in infant lung function testing • Flow-volume pattern • Flow-time pattern • Rather often adaptation of interpretation strategies from adults V.P. Seppä et al. Tidal breathing flow measurements in awake young children by using impedance pneumotachography. J ApplPhysiol. 2013; 115: 1725-1731
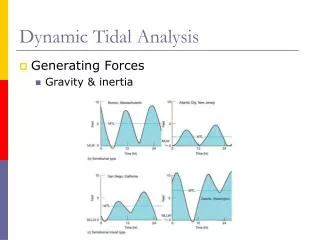
Tidal breathing analysis in practice (adults) Adult subject (a) Normal / obstructive ? Adult subject (b) Normal / obstructive ?
Tidal breathing in spirometry Subject (a) Emphysema Subject (b) Healthy
“Contra” tidal breathing analysis • Variability • Freedom of the subject to breath slower, faster, deeper or more shallow • No standards for achieving reproducibility • In the past: Metronome; BF=constant • Sensitivity and specificity of flow pattern • Nearly all respiratory problems lead to flow limitation • Only severe degrees of disability become visible • Usually more complex technology needed • Specific quality, best selection and classification concepts
Specific methods for (clinical) evaluation • Problems: • Standardisation of breathing • Intra-breath variability • Limitations not yet visible at tidal breathing • Flow-volume pattern ambiguous • Solutions: • Statistical methods for evaluation • Long term recording • Individual trend analysis • Pre-post assessment • Intra-breath variability of 2 flow-volume-parameters: • Tpef%Tex • Vpef%Vex Still the flow-volume recording of tidal breathing lacks information!
Survay of methods (applications) Flow (volume) in combination with one ore more additional signals (simultaneous recording) • Rint, Rocc Occlusion pressure - Pint/Pocc • sRaw, Bodyplethysmography - Vshift • R5, X5, Oscillometry - Pmouth (ext. generator) • P0.1 Breathing pump - Pint/Pocc • FRCHe, FRC-Rebreathing - %He • Cdyn, Compliance - Poes • CO2/O2, Capnography/Oxymetry - %CO2/O2 • RAAR, Rhinomanometry - Pchoanae • Wheezing, Lung sound analysis - Sound • Zimp, Impedance tomography - Impedance
FRC-stability (EEL) • Common long term stability of flow channel > 5 min • Offset of flow transducer stays within “dead zone” • New, high stable and temperature compensated pressure transducers Volume drift upwards • Physiologic criteria for FRC-stability • Regularity of breathing • BF constant • VT constant FRC-stability line Volume drift downwards
Sources of drift • Drift of volume is an technical issue – ATP-BTPS correction • It is not possible to eliminate this drift • In future statistical methods • Sources of drift • Approximation of ATP-BTPS correction • Correction depends / varies with: • Changes in ATP • Use of filters • Breathing pattern (flow profile) • Ratio of dead space / alveolar ventilation • Adaptation of Patient • Calibration • Solution • Post processing • Depending on measurement application • Applied on specific breaths or entire recording • Excludes physiological changes of EEL • Visual inspection of adaptation • Offset correction Volume drift
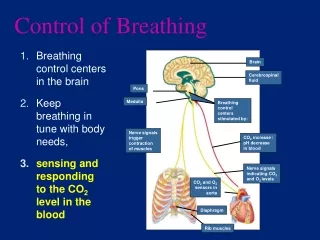
Repeatability (within trial / between tests) Standardisation ? • Patient has all degrees of freedom to increase, lower VT, BF • What is the standard? In the past • Standardization of BF – Metronome • Need of corrective action of patient • Shift of FRC Nowadays • Non-restricted spontaneous breathing is requested • Confirmation of normal resting breathing • The point of lowest WOB is highly reproducible Respiratory system always tries to minimise WOB • Regulation / optimisation of BF and VT Obstruction BF i, VT hRestriction BF h, VT i
Decreasing variability of measurement • Edit capabilities • Selection, deselection • Manual corrections • Resultc Subjective influence increases variability of results
Reliable concepts to improve quality • Adaptation phase until regular tidal breathing • Familiarisation with mouth breathing through instrument • Instruction/confirmation of spontaneous breathing (at individual lowest WOB) In case of insufficient cooperation • Increase of number of breathing cycles • Increase of number of trials • Repeated recording after optimised instruction • Rejection of artefact affected trials • Editing artefact effected trials is not recommended !
BEST selection in tidal breathing analysi • Maximum / Minimum • Not applicable in tidal breathing analysis • Median (usually) • Arranging all the observations from lowest value to highest value and picking the middle one • Advantage: Robust against artefacts • Disadvantage: BEST as good as single trial • Average • Sum of a list of numbers divided by the size of the list • Advantage: Improves with number of trials BEST is better than a single trial • Disadvantage: Strongly effected by artefacts • Use requires prior artefact rejection
Comparisonof median – meancalculation Low variability of sReff (Reff, TGV)and FRC Median = mean
Full body plethysmography Characteristic and clinical usefulness / interpretation of breathing (resistance) loops.
Breathing loop without Raw 0 Flow [L.s-1] Flow sReff DVm 0 Shift volume Shift volume [mL] TGV DVth DVthorax = DVmouth No compression / decompression of air in lungs. Movement of thorax is NOT detected by box! No Shift volume!
Breathing loop with Raw >> 0 Flow Flow [L.s-1] sReff Fraction Raw sReff DVm Raw>> Alveolar pressure >> 0 + PA + Shift volume Compression / decompression DVth Sift volume [mL] Shift volume= proportional to Raw
Breathing loop with Raw >> & TGV 0 Flow Flow [L.s-1] Fractions RawTGV DVm Raw>> sReff + PA + Alveolar pressure >> 0 Shift volume Compress. / decompress. TGV DVth Sift volume [mL] Shift volume=further increased by TGV Alveolar pressure = constant!
Summary - breathing loop Specific resistance (sRaw) incorporates (Raw, TGV) Flow [L.s-1] • sRaw breathing loop • Specific Resistance • Related to WOB, efforts for breathing • Without shutter measurement! • Proportional to Raw and TGV • Not a resistance loop! (Alveolar pressure ~ Raw only) Pecularitiesof the sRaw breathing loop • Low variability as primary measure • High clinical relevance / significance • Answer on relevant clinical questions: abnormality, local distribution, reversibility, hyperresponsiveness sReff Parameters sRtot Shift volume [mL]
Weibel: Morphometry of the human lung Cross sectional area [cm²] 2.5 2.0 5.0 1.8 x 10² 9.4 x 10² 5.8 x 10³ 56 000 000 Resistance [kPa/(L/s)] 0.05 0.05 0.02 Genera- tion 8-10 17 24 Larynx Trachea Bronchi Bronchioles Alveolar Ducts Alveoli Central airways R ~ 80% Peripheral airways R < 20% TGV > 60 % Weibel, Morphometry of the Human Lung, Springer 1963
Raw-TGV dependency Raw > Raw < TGV < TGV > = sRaw = Rawhigh & TGVlow Rawlow & TGVhigh Specific Resistance (sRaw) • Normalises airways resistance to lung volume • Low dependence on biometrical data • Reference values are constant
Clinical information based on sRaw Threshold to abnormal lung function • Adults sRaw > 1.2 kPa.s (Raw & TGV) • Children sRaw > 1.0 kPa.s (Raw & TGV) Reversibility • No…………No significant change of sRaw • Partial…….Significant decrease of sRaw • Complete….sRaw becomes normal Hyperresponsiveness • PD/C+100sRaw & > 2.0 kPa.s • PD/C-40sGaw & < 0.5 kPa-1.s-1 Important clinical questions are answered based on tidal breathing! Incorporating the entire respiratory tract. Flow V‘ [L.s-1] Clockwise turn sReff Approximation TGV Reff Shift volume [mL]
Differential diagnsotics via sRaw- loop Degree of opening, separately for in- and expiration K1 closed, steepc Normal lung function K2 little opened, clockwise turned cCentral obstruction K3 Golf club cPeripheral end-expiratory inhomogeneity K4 V-shapecElevated diaphragm and/or end-expiratory „closing“ K5 Markable S-shapecExtra thoracic stenosis
Impulse Oscillometry New multiple trial concept.
Tidal breathing analysis • Spontaneous breathing pattern • Physiologic, effortless, patient friendly • No age limitation • Highly reproducible (Point of lowest WOB) • Variety of different methods available • Global information (sReff) • Highly differentiated (Raw, FRC; R5, X5) • New concepts for artefact elimination • Median >> automated artefact rejection and mean calculation