Download

1 / 70
700 likes | 794 Views
Introduction to Pro-Inflammatory Therapy. What is it? What is the evidence?. Kevin deWeber , MD, FAAFP, FACSM Military Sports Medicine Fellowship Bethesda, MD And Keith A Scorza , MD, MBA August 2012. Objectives. Historical Perspectives Review the theoretical basis

E N D
Introduction to Pro-Inflammatory Therapy What is it? What is the evidence? Kevin deWeber, MD, FAAFP, FACSM Military Sports Medicine Fellowship Bethesda, MD And Keith A Scorza, MD, MBA August 2012
Objectives • Historical Perspectives • Review the theoretical basis • Review Current Evidence • Review our own clinical experience
Terminology • Prolotherapy: proliferative therapy • Generally used to refer to “traditional” agents • Pro-inflammatory therapy: broader term including injections that increase inflammation and hopefully increase healing • Prolotherapy • Blood or Platelet-Rich Plasma • ?dry needling
Historical Definitions Injection of a solution…that will stimulate the production of new cells. George S Hackett, 1956 Injection of growth factors or growth factor stimulants…that causes growth of normal cells or tissues Reeves, KD and Hassanein KM 2000/2003
Early Prolotherapy First described in 1937 by Dr Louis Schultz Injected sodium psylliate into painful tempomandibular joints Written about by Dr. George Hackett, 1956
Acute Injury Healed Tissue Chronic Degeneration or Tendinopathy
Sports Medicine Dogma • Make the Diagnosis • Control pain and Inflammation • Control abuse • Rehabilitative exercise • Return to Function
Controlling Inflammationin the traditions of sports medicine • NSAIDs • Proven anti-inflammatory, analgesic • Down-sides: • Adverse GI, renal effects • Suppression of normal inflammatory healing cascade • Corticosteroids • Proven anti-inflammatory, analgesic • Down-sides: • Tissue atrophy • Increased risk of tears • Doesn’t promote healing; slows it down
Ekeberg OM et al. Subacromial ultrasound guided or systemic steroid injection for rotator cuff disease: randomised double blind study. BMJ 2009WITH CORTICOSTEROIDS… =
Coombes BK, Bisset L, Vicenzino B. Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: a systematic review of randomised controlled trials. Lancet 2010 Nov 20;376(9754):1751-67Hart L. Corticosteroid and otherinjections in the management of tendinopathies; a review. Clin J Sport Med 2011 No . • Corticosteroids: • Short-term ( 4 weeks) • analgesia proven • Intermediate and long-term (12-52 weeks) • WORSE THAN OTHER INTERVENTIONS
So why not try to promote healing FIRST by letting/helping inflammation do its job???PROLOTHERAPY
Prolotherapy Agents Traditional Agents • Irritants • Phenol, guaiacol, tannic acid • Osmotics • Dextrose, glycerin • Chemotactics • Sodium morrhuate • Particulates • Pumice flour
Prolotherapy Agents Newer Agents Growth factors Whole blood Platelet-rich plasma (PRP) Platelets…they’re not just for clotting anymore…
Platelet Alpha Granules Platelet-derived growth factor (PDGF) Transforming growth factor (TGF) Vascular endothelial growth factor (VEGF) Epidermal growth factor (EGF) Fibroblast growth factor (FGF)
Prolotherapy The basic science
In Vitro Studies:Traditional Agents Cells bathed in traditional agents have shown increased expression of genes for inflammation and growth factors
In Vitro Studies:Blood Products Cells bathed in blood products have shown: • Increased cell proliferation • Increased gene expression • Increased cartilage production
Animal Studies:Traditional Agents • Soft tissue fibrosis • Increases in tendon diameters • Ligament hypertrophy and strength
Animal Studies:Blood Products Repair of cartilage tears Increased tendon strength Healing of OCD’s Improved muscle healing
Prolotherapy What is the evidence In HUMAN studies?
Overview of the evidence • Limited in number, but growing • Many case series, few RCTs • Overall, promising results
Major Primary Care Interests • Patellar Tendinopathy • Lateral epicondylopathy (Tennis Elbow) • Achilles Tendinopathy • Rotator Cuff Tendinopathy and partial tears • Plantar Fasciopathy • Osteoarthritis • Sacro-Iliac Joint Pain • Lower Back Pain • Then we’ll examine a few other areas of interest
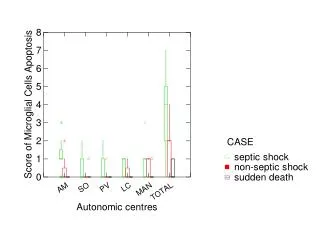
Results Key • Green: improvement; or better than placebo • White: no improvement OR same as placebo • Red: worsened OR worse than placebo
Elbow epicondylopathy • Traditional Therapies • Zeisig et al. 2006 series • Scarpone et al. 2008 RCT • Carayannopoulos 2011 RCT • Autologous Blood • Edwards/Calandruccio 2003 series • Connell et al. 2006 series • Suresh et al. 2006 series • Ozturan et al 2010 RCT • Kazemi et al 2010 RCT • PRP • Mishra and Pavelko 2006 series • Peerbooms et al, 2010 RCT • Creaney et al 2011 RCT, ABI = PRP • Hechtman et al 2011 series
Lateral epicondylopathy RCTCarayannopoulos et al 2011 • N=24, Dextrose vs steroid • Injections 0 & 4 weeks • BOTH treatments: LESS PAIN at 3 and 6 months • BOTH: HIGHER FUNCTION at 3 and 6 months • No significant differences between groups • underpowered =
Lateral epicondylopathy RCTOzturan et al 2010 • N=60 • Steroid v. Blood v. ShockWave • Injections: ONE time Percent “success” <
Lateral epicondylopathy RCTKazemi et al 2010 • N=60, Steroid v. Blood • SINGLE Injection • Outcomes: • Grip strength • Pain • Function • Disability • tenderness • 4 weeks: BOTH BETTER • BLOOD better than steroid on pain, grip, disability, tenderness • 8 weeks: BLOOD better in ALL outcomes >
Lateral epicondylopathy RCTPeerbooms et al 2010 • N=100 • Steroid v. PRP • SINGLE Injections • Outcomes at 1 year • DASH disability • VAS pain • Success: >25% better Percent “success” <
So, for tennis elbow, at one year after treatment… • Blood is better than steroid • PRP is better than steroid • Which is better: blood or PRP??
Lateral epicondylopathy RCTCreaney et al 2011 • N=150 • Blood v. PRP • Injections: 0 & 1 month • Outcome: Pt-Related Tennis Elbow Eval (PRTEE) @6mo Percent “success” =
Patellar tendinopathy • Traditional Prolotherapy • Haksrud et al. 2006 series • Ryan et al. 2011 series • PRP • Kon et al. 2009 series • Filardo et al. 2009 case/control • Gosenset al 2012 series Image from: Fullerton BD. High-resolution ultrasound and magnetic resonance Imaging to document tissue repair after prolotherapy: a reportof three cases. Arch Phys Med Rehabil 2008;89:37-85.
Achilles Tendinopathy Traditional Prolotherapy Yelland et al. 2011 RCT PRP Case Series Sanchez et al. 2005 Sanchez et al 2007 Gaweda et al 2010 Monto 2012 RCT de Vos et al. 2010 RCT No eccentric training prior!
Achilles tendinopathy RCTYelland et al 2011 • N=43, Dextrose vsEccentricExvs COMBO • Success = 20-pt fall in VISA-A at One Year • Dextrose and COMBO: • FASTER RESULTS • One Year: No significant differences between groups • underpowered
Achilles Tendinopathy RCTdeVos et al 2010, 2011 • No prior eccentric exercises!! • Saline vs PRP, n=54 • Both groups received EccEx • Equal results at 24 and 52 months • Faulty study design
Plantar Fasciopathy • Autologous Blood Inj (ABI) • Lee and Ahmad 2007 DB-RCT vs CSI • Kalaci et al. 2009 RCT vs CSI • PRP • Barrett/Erredge 2004 series • Peerbooms: RCT underway
Plantar Fasciopathy RCTLee/Ahmadet al 2007 • N=63 • Blood • Steroid • Both groups improved • 6 weeks: STEROID better • 3 months: STEROID still better • 6 months: EQUAL =
Plantar Fasciopathy RCTKalaci et al 2009 • N=100, 4 groups • Blood • Steroid • Lidocaine + “peppering” • Steroid + “peppering” • NEEDLE FENESTRATION • All groups better @6mos • Best: Steroid + peppering (P<.05)
Plantar Fasciopathy RCTAksahin et al 2012 • N=60, 2 groups • PRP • Steroid (40 Mg Mpred) • All groups equally better @3 weeks and 6 mos =
Rabago D et al. A systematic review of prolotherapy for chronic musculoskeletal pain. Clin J Sports Med 2005;15(5) Lower Back(Traditional agents) • RCTs • Ongley et al. 1987 (PGG) • Klein et al. 1993 (PGG) • Dechow et al. 199 (PGG) • Yelland et al 2004 (20% dext) • Non-randomized Studies • Yelland et al 2000 (dext) • Series • >22 series published 2004 • Watson 2010 • Cusi at al 2010
Sacroiliac Joint • Kim at al 2010 RCT (dextrose) • Naeim et al 1982 non-randomized trial (dextrose) • Cusi 2008 series (SI jt, dextrose)
Sacroiliac Joint RCTKim et al 2010 • N=48, pain >3 months • PROVEN Pain relief w/ intra-articular lido • Steroid v. Dextrose • Injections q2wks, max 3 • Outcome: • Success - >50% pain relief at 15 months Percent “success” <
Knee Osteoarthritis • Traditional prolo • Reeves & Hassanein 2000 RCT • Rabago et al, 2012 series • PRP • Sanchez et al. 2008 case/cont • Knee OA, PGRF vshyaluronan • Kon 2010 and Filardo 2011, series • Sampson et al 2010 series • Wang-Saegusa et al 2011 series • Filardo at al 2011 series • Gobbi et al 2012 series • Kon/Mandelbaum et al. 2011 PRP vsVisco • Spakova et al 2012 PRP vsVisco • Patel et al 2013 PRP vs placebo Image from: Sun Y, Feng Y, Zhang CQ et al. The regenerative effect of platelet-rich plasma on healing in large osteochondral defects. International Orthopedics 2009. Online April 18, 2009
Knee Osteoarthritis Prolo, RCTReeves, Hassanein 2000 • N =38 • 10% dextrose+lidiovs lido • 9cc every other month x6months • Outcomes @6 mos: • Pain • Swelling • bucking • Outcome @12mos: • radiographs • Dextrose benefits • 44% less PAIN • 63% less SWELLING • 85% less BUCKLING • Xrays @12 mos: thicker lat PFJ cartilage! >
Knee Osteoarthritis PRP: RCTKon/Mandelbaum et al 2011 • 150 pts, early to sev OA • 50 pts: 3 PRP inj’s • 50 pts: High-MW HA • 50 pts: Low-MW HA • 2 months: PRP and LMW-HA better than HMW-HA • 6 months: PRP best • Pts over 50 yrs: PRP = HA • Pts under 50: PRP best
Knee Osteoarthritis PRP: RCTSpakova et al 2012 • Non-blinded, 120 pts • Weekly inj x 3 • PRP 4.5x plt w/ leuk • HA (Erectus, med MW) • WOMAC at 3 & 6 mos • 3 mos: both signif better • PRP signif better than HA • 6 mos: both still better • PRP signif better than HA
Knee Osteoarthritis PRP: DB, PC-RCTPatel et al 2013 • DB-RCT • 78 pts w bialt OA (156 knees) • 26 PRP x1 • 25 PRP at wks 0 and 3 • 23 saline • WOMAC and VAS pain at 3 wks, 3 and 6 mos • PRP was leuk-free, 3x plt • 3 wks: both PRP grpssltly better • 3 mos: both PRP grps markedly better, saline worse • 6 mos: both PRP grps still markedly better (slt regression), saline worse