Download
1 / 56
610 likes | 894 Views
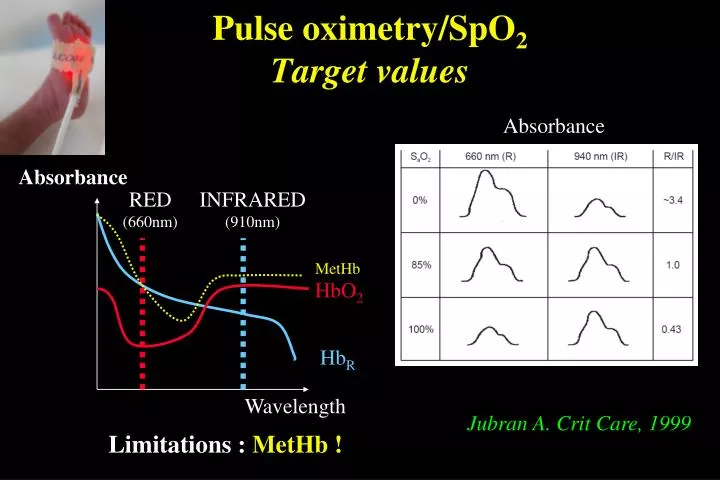
Pulse oximetry/SpO 2 Target values. Absorbance. Absorbance. RED (660nm). INFRARED (910nm). MetHb. HbO 2. Hb R. Wavelength. Jubran A. Crit Care, 1999. Limitations : MetHb !. Target SpO 2 ?. BOOST Trial (Askie LM et al. NEJM, 2003). Aim the study

E N D
Pulse oximetry/SpO2Target values Absorbance Absorbance RED (660nm) INFRARED (910nm) MetHb HbO2 HbR Wavelength Jubran A. Crit Care, 1999 Limitations : MetHb !
Target SpO2 ? • BOOST Trial (Askie LM et al. NEJM, 2003) Aim the study To compare targets SpO2 : 91-94% vs 95-98% Population Preterm infants < 30 weeks GA O2 dependant at 32 weeks PCA End-Point Chronic Lung Disease Neurodevelopmental outcome at 12 months
N=358 SpO2 95-98% N=180 SpO2 91-94% N=178 CLD (36 w) 46% 64%* Home O217% 30%* Duration O217d 40d* Death 3% 5% Askie LM et al. NEJM, 2003
N=358 At the age of 12 months SpO2: 95-98% N=180 SpO2: 91-94% N=178 Major neurodevelopmental anomalies 24% 23% Weight 9.1 kg 9.2kg Askie LM et al. NEJM, 2003
Target SpO2 ? • BOOST Trial (Askie LM et al. NEJM, 2003) • STOP-ROP study (Pediatrics, 2000) Aim of the study To compare target SpO2 : 89-94% vs 96-99% Population Preterm infants with Retinopathy End-Point ROP Chronic Lung Disease
N=649 SpO2 96-99% N=325 25.4 weeks 35.4 SpO2 89-94% N=324 GA=25.4 weeks PCA=35.3 ROP progression 48% 41% At 3 months corrected age : hospitalization 6% 12%* Death 3% 5% Pediatrics, 2000
Target SpO2 ? • BOOST Trial (Askie LM et al. NEJM, 2003) • STOP-ROP study (Pediatrics, 2000) Summary 1 Compared with target SpO2 96-99%, target SpO2 between 89 and 94% reduces the risk of CLD, duration of O2 therapy, and home O2 need… … but what about lower SpO2 target ?
Target SpO2 ? • BOOST II Trial, NEJM 2013 Aim the study To compare targets SpO2 : 85-89% vs 91-95% Population Preterm infants < 28 weeks GA (N=2448) To 36 weeks PCA End-Point Disability-free survival
Target SpO2 ? B Schmidt, JAMA 2013 Aim the study To compare targets SpO2 : 85-89% vs 91-95% Population Preterm infants < 28 weeks GA (N=1201) To 36-40 weeks PCA End-Point Death or Disability at age 18 months
Take home message In preterm infants < 28 weeks GA : • SpO2 > 96 est associée à : • CLD • O2 duration • ROP • Hyperoxemia can occur with SpO2 target between 90-96%; • SpO2 < 89% est associée à: • mortality ( NEC ?) • ROP Target SpO2 between 89 and 96 %
Dates à retenir ! • Le 14 Février 2014 de 9h à 18h : Formation EIRENE/GEN aux Soins Palliatifs (Inscription nécessaire); • Le 5 Juin 2014 à Rouen : 9ème Journée Paramédicale du G4 en Médecine Néonatale; • Le 12 Juin 2014 à Roncq, Amphytrion : 5ème réunion commune Collège Obstétriciens / GEN • Le 19 Juin 2014 à Lille: Journée Régionale de Pédiatrie
Target SpO2 ? • SpO2 Hyperoxemia can occur with SpO2 target between 90-96%; • Physiologic evidence suggest that O2 delivery can be normal when SpO2 is lower than 88%, providing adequate cardiac output and hemoglobin concentration ; • Clinical data suggest that target SpO2 between 70 and 90% reduces ROP, O2 need without increasing neurological impairment in very preterm infants.
Absorbance Pulsatile blood flow (arterial) Elimination of the nonpulsatile component of the absorbance No pulsatile blood flow (venous, capillary) Tissue (myoglobin, bone…) Time Red/Infrared Absorbance (SpO2) + distal perfusion index Limitations : Low distal perfusion ! = SvO2
Evidence for a benefit of SpO2 < 90-95% in the preterm infant ? Jubran A. Crit Care, 1999 • Physiologic data • Evidence for deleterious effects of high PaO2 (>80mmHg?) • Increase the risk of ROP and respiratory morbidity (Askie LM. Cochrane, 2001) • Risk of hyperoxemia with SpO2 range 90-95% ? SpO2 95 90 PaO2 (mmHg) 42 110
Evidence for a benefit for SpO2 < 90-95% in the preterm infant ? • Physiologic data • Components of the tissue oxygenation Fetal circulation PaO2 = 18 mmHg ! SaO2 = 60 % !
O2 delivery = 1.3 x AoFlow x Hb x SpO2 PvO2 O2 consumption
Anaerobic metabolism Aerobic metabolism EO2 VO2 Lactate PvO2 PvO2 O2 Delivery = 1.3 x AoFlow x Hb x SpO2 Critical DO2
Evidence for a benefit for SpO2 < 90-95% in the preterm infant ? 1. Physiologic data • Lack of evidence for hypoxia in hypoxemic preterm infants (Petrova A et al. Pediatr Crit Care Med, 2006) • Prospective study • 10 preterm infants 24-32 weeks GA • Mesurement of tissular oxygenation (NIRS, brain and kidney) when SpO2 < 80% ; No tissular hypoxia (Tissular SO2 and Fractional O2 Extraction : Adequate)
Evidence for a benefit for SpO2 < 90-95% in the preterm infant ? 2. Clinical data • Tin W et al. Arch Dis Child Fetal Ed, 2001 • Retrospective study • 295 preterm infants < 28 weeks GA • Comparison of different policies : Target SpO2 70-90% vs 88-98%
Outcome of the preterm infants according to the policy of target SpO2 Tin W et al. Arch Dis Child Fetal Ed, 2001
Respiratory outcome Tin W et al. Arch Dis Child Fetal Ed, 2001
Evidence for a benefit for SpO2 < 90-95% in the preterm infant ? 2. Clinical data • Deulofeut R et al. J Perinat, 2006 • Retrospective study • Comparison of 2 historical periods : • 2000-2002 : Target SpO2 92-100% • 2003-2004 : Target SpO2 85-92% 502 preterm infants < 1250g Period 2003-2004 : • Less ROP • Less CLD • Higher Mental Developmental Index (89 vs 80)
Target SpO2 : Pre- and/or Post ductal ? Persistent Pulmonary Hypertension Of the Newborn/Preterm : • Premature Rupture of the Membranes • Sepsis • Severe HMD RA RV LV Pre-ductal : higher SpO2 DA PA Post-ductal : lower SpO2 DO2= 1.3 x AoFlow x Hb x SpO2
Target SpO2 : Pre- and/or Post ductal ? In the premature infant, Pre-ductal SpO2 should be used to set FiO2 ! RA RV LV Pre-ductal : higher SpO2 DA PA Post-ductal : lower SpO2 DO2= 1.3 x AoFlow x Hb x SpO2
Target PCO2/TcPCO2 ? Evidence for adverse effects of low PCO2 < 35mmHg • Increase the risk of BPD/CLD (Avery ME et al Pediatrics 1987. Garland et al Arch Pediatr Adolesc Med, 1995); • Increase the risk of Periventricular Leucomalacia (Graziani LJ, et al. Pediatrics 1992. Fujimoto S, et al. Arch Dis Child 1994);
Premature infants 400 à 1200 g Severe IVH N=179 No severe IVH N=670 PaCO2 in the first 4 days after birth Pediatrics 2007;119:299
Effects of the fluctuations of PaCO2 on the risk of IVH Fabre J et al. Pediatrics 2007;119:299
Target PCO2 ? Summary 1 Adverse lung and brain effects of : • Low PCO2 <35 mmHg ; • Fluctuating PCO2
Target PCO2/TcPCO2 ? 2. Evidence for beneficial effects of moderate hypercapnia 45-55 mmHg Premature infants 600 à 1200 g, < 24 hrs MV Target PCO2 35-45 mmHg N=24 26 weeks 850 g 45-55 mmHg N=25 26 weeks 850 g End-point : Duration of mechanical ventilation Mariani. Pediatrics, 1999
Actual values of PaCO2 according the target PaCO2 Mariani. Pediatrics, 1999
Effects of the target PaCO2 on the peak inspiratory pressure Mariani. Pediatrics, 1999
Effects of the target PaCO2 on the duration of MV Mariani. Pediatrics, 1999
Effects of the target PaCO2 on the nonrespiratory outcomes Mariani. Pediatrics, 1999
Target PCO2/TcPCO2 ? 3. Why not > 55 mmHg ??? Premature infants 400 à 1200 g Severe IVH N=176 No severe IVH N=670 PaCO2 in the first 4 days after birth Fabre J et al. Pediatrics 2007;119:299
Target SpO2 / PCO2 in the preterm infant ? Back home message SpO2 : • Preductal SpO2, instead of postductal, should be monitered during the first days after birth; • Target SpO2 should not be > 95% : • Target SpO2 < 92% may be preferred in extremely preterm infants
Target SpO2 / PCO2 in the preterm infant ? Back home message PCO2: • Special care should be taken to prevent hypocapnia (<35 mmHg) and acute fluctuations of PCO2; • Moderate hypercapnia (45-55 mmHg) is associated with lower morbidity than normal PCO2; • Too much of a good thing (CO2) may cause adverse cerebral effects, at least within the first few days of life (PaCO2 > 60 mmHg) !
Hypotension : • Preterm : AoP < GA + 2 mmHg/d, until 35 mmHg ; • Full-term : AoP < 40 mmHg ;
aEEG Ischemic Threshold ? CBF Kissack, Pediatr Res 2004 Victor, Pediatr Res 2006
La PA n’est pas la perfusion 45 preterm infants <1500g Age <36h Mechanically ventilated No DA ou <1.5mm Kucklow M, J Pediatr. 1996 Pladys P, Eur J Pediatr. 1999
O2 Delivery =1.3 x Qc x Hb x SpO2 AoP = Qc x SVR Systemic Vascular Resistances (SVR) Systemic Blood flow (Qc) Preload Contractility Afterload Heart Rate Tibby SM, Arch. Dis. Child. 2003