Download
1 / 17
200 likes | 422 Views
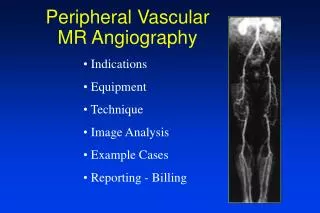
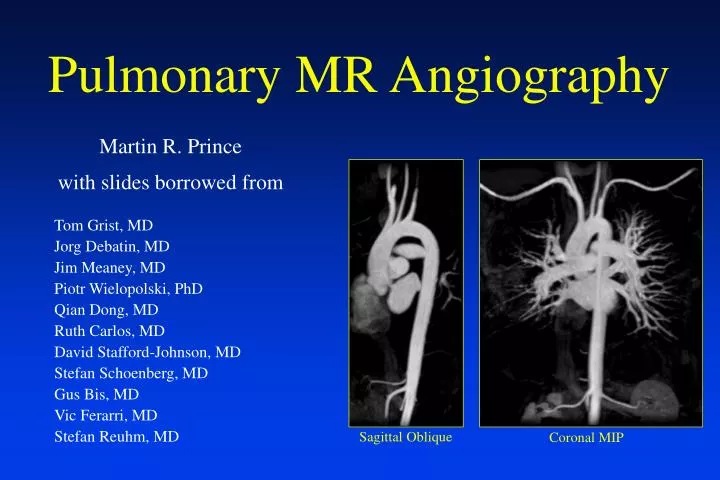
Sagittal Oblique. Coronal MIP. Pulmonary MR Angiography. Martin R. Prince with slides borrowed from. Tom Grist, MD Jorg Debatin, MD Jim Meaney, MD Piotr Wielopolski, PhD Qian Dong, MD Ruth Carlos, MD David Stafford-Johnson, MD Stefan Schoenberg, MD Gus Bis, MD Vic Ferarri, MD

E N D
Sagittal Oblique Coronal MIP Pulmonary MR Angiography Martin R. Prince with slides borrowed from Tom Grist, MD Jorg Debatin, MD Jim Meaney, MD Piotr Wielopolski, PhD Qian Dong, MD Ruth Carlos, MD David Stafford-Johnson, MD Stefan Schoenberg, MD Gus Bis, MD Vic Ferarri, MD Stefan Reuhm, MD
Pulmonary Embolism • > 600,000 per year • 30% mortality • Difficult to diagnosis • V/Q - 64% indeterminate • Angio is expensive + risks • CTA safer but nephrotoxicity • Anticoagulation: 7% risk of • major complication
Coronal 3D Volume • image both lungs simutaneously • large dose of Gd • (<180 lb 2 bottles, 42ml) • (>180 lb 3 bottles, 63ml) • one injection • Sagittal 3D Volumes • small FOV, no wrap • two separate injections • main PA excluded MR Angiography Protocol Coronal 3D Gd:MRA
Pulmonary MRA Technique • Sagittal Locator 1 min • Coronal 3D Volume x 3 1.5 min • Total imaging time <3 min
Prescribing Coronal 3D Volume • Posterior to spinal cord • Anterior to the ascending aorta • Large FOV to prevent wrap • No spoiling • Fast scan for breath holding • Thick slices: 3-5 mm • Zero interpolation (ZIP x 2) • Gradient upgrade for short TR • Partial Fourier Imaging • Multiphase
Injecting the Gadolinium • 2 ml/sec (as fast as you can) • 6-10 second scan delay for • arterial phase • equilibrium phase • rest to catch breath • equilibrium phase again • ventilated patient: suspend • in max inspiration Arterial Phase Equilibrium Phase
Pulmonary Embolism:Diagnosis with MRA Author Year # of pt Techniques Sensitivity Specificity Grist 1993 20 TOF 92% 63% Isoda 1995 18 3D Gd 80% 95% Laissy 1995 28 TOF + Gd 87% 95% Wolff 1996 34 2D Gd 72% 94% Meaney 1997 30 3D Gd 87% 97% Gupta 1999 36 3D Gd 85% 96%
Diagnosis of Pulmonary Embolism* with MRA (n=30) 1 2 3 Sensitivity 100% 87% 75% Specificity 95% 100% 95% *Meaney et al. NEJM 366:1422-7, 1997.
Diagnosis of Pulmonary Embolism* with MRA (n=36) Reviewer 1 2 Sensitivity 92% 77% Specificity 83% 91% PPV 75% 83% NPV 95% 88% *Gupta et al Radiology 1999; 210:353-359
Shortness of Breath with cough in a 51-year-old female Magnification Reformation Coronal MIP
Partial anomlous pulmonary venous return from the right upper lobe Magnification Reformation Coronal MIP
Patent Ductus Arteriosus Axial T1
Summary • 3D Gd:MRA useful • Safe • no nephrotoxicity • no ionizing radiation • no arterial catheterization • Fast (30 second breath hold) • Accurate • Better with blood pool? Blood pool agent MRA