Download
1 / 1
10 likes | 168 Views
WCO-IOF- ESCEO. EQ-5D AND QUALITY OF LIFE OF OSTEOPOROSIS AT-RISK PATIENTS IN A SWEDISH OSTEOPOROSIS PATIENT REGISTRY Arun Krishna 1 , Dan Mellström 2 , Zhiyi Li 3 , Chun-Po Steve Fan 3 , Stina Salomonsson 4 , Ewa Waern 2

E N D
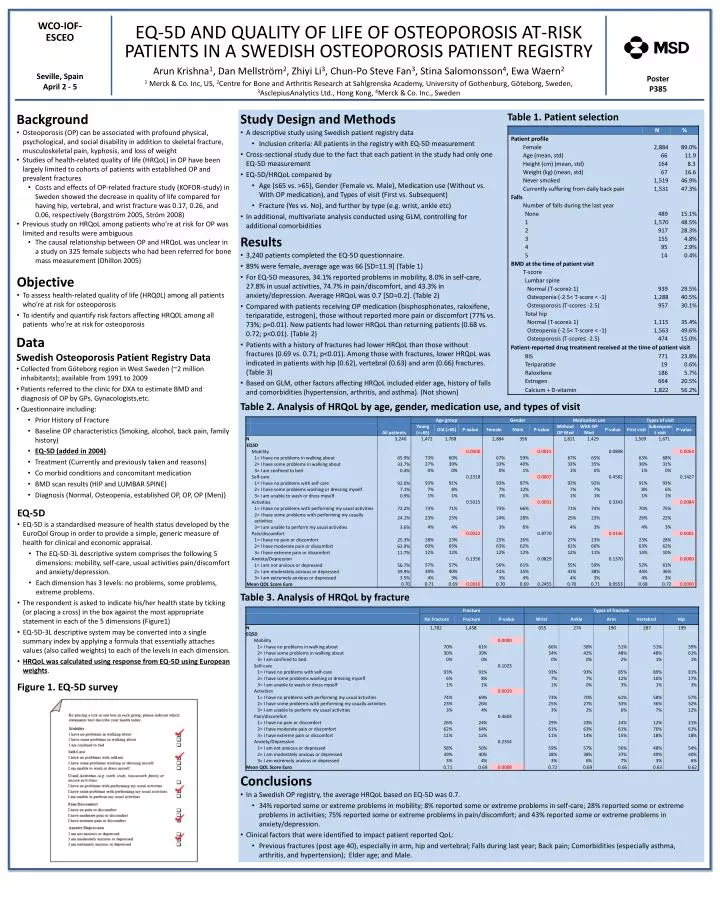
WCO-IOF- ESCEO EQ-5D AND QUALITY OF LIFE OF OSTEOPOROSIS AT-RISK PATIENTS IN A SWEDISH OSTEOPOROSIS PATIENT REGISTRY Arun Krishna1, Dan Mellström2, Zhiyi Li3, Chun-Po Steve Fan3, Stina Salomonsson4, Ewa Waern2 1 Merck & Co. Inc, US, 2Centre for Bone and Arthritis Research at Sahlgrenska Academy, University of Gothenburg, Göteborg, Sweden, 3AsclepiusAnalytics Ltd., Hong Kong, 4Merck & Co. Inc., Sweden Seville, Spain April 2 - 5 Poster P385 Table 1. Patient selection • Background • Osteoporosis (OP) can be associated with profound physical, psychological, and social disability in addition to skeletal fracture, musculoskeletal pain, kyphosis, and loss of weight • Studies of health-related quality of life (HRQoL) in OP have been largely limited to cohorts of patients with established OP and prevalent fractures • Costs and effects of OP-related fracture study (KOFOR-study) in Sweden showed the decrease in quality of life compared for having hip, vertebral, and wrist fracture was 0.17, 0.26, and 0.06, respectively (Borgström 2005, Ström 2008) • Previous study on HRQoL among patients who’re at risk for OP was limited and results were ambiguous • The causal relationship between OP and HRQoL was unclear in a study on 325 female subjects who had been referred for bone mass measurement (Dhillon 2005) Study Design and Methods • A descriptive study using Swedish patient registry data • Inclusion criteria: All patients in the registry with EQ-5D measurement • Cross-sectional study due to the fact that each patient in the study had only one EQ-5D measurement • EQ-5D/HRQoL compared by • Age (≤65 vs. >65), Gender (Female vs. Male), Medication use (Without vs. With OP medication), and Types of visit (First vs. Subsequent) • Fracture (Yes vs. No), and further by type (e.g. wrist, ankle etc) • In additional, multivariate analysis conducted using GLM, controlling for additional comorbidities • Results • 3,240 patients completed the EQ-5D questionnaire. • 89% were female, average age was 66 [SD=11.9] (Table 1) • For EQ-5D measures, 34.1% reported problems in mobility, 8.0% in self-care, 27.8% in usual activities, 74.7% in pain/discomfort, and 43.3% in anxiety/depression. Average HRQoL was 0.7 [SD=0.2]. (Table 2) • Compared with patients receiving OP medication (bisphosphonates, raloxifene, teriparatide, estrogen), those without reported more pain or discomfort (77% vs. 73%; p=0.01). New patients had lower HRQoL than returning patients (0.68 vs. 0.72; p<0.01). (Table 2) • Patients with a history of fractures had lower HRQoL than those without fractures (0.69 vs. 0.71; p<0.01). Among those with fractures, lower HRQoL was indicated in patients with hip (0.62), vertebral (0.63) and arm (0.66) fractures. (Table 3) • Based on GLM, other factors affecting HRQoL included elder age, history of falls and comorbidities (hypertension, arthritis, and asthma). (Not shown) Objective • To assess health-related quality of life (HRQ0L) among all patients who’re at risk for osteoporosis • To identify and quantify risk factors affecting HRQ0L among all patients who’re at risk for osteoporosis Data Swedish Osteoporosis Patient Registry Data • Collected from Göteborg region in West Sweden (~2 million inhabitants); available from 1991 to 2009 • Patients referred to the clinic for DXA to estimate BMD and diagnosis of OP by GPs, Gynacologists,etc. • Questionnaire including: • Prior History of Fracture • Baseline OP characteristics (Smoking, alcohol, back pain, family history) • EQ-5D (added in 2004) • Treatment (Currently and previously taken and reasons) • Co morbid conditions and concomitant medication • BMD scan results (HIP and LUMBAR SPINE) • Diagnosis (Normal, Osteopenia, established OP, OP, OP (Men)) Table 2. Analysis of HRQoL by age, gender, medication use, and types of visit EQ-5D • EQ-5D is a standardised measure of health status developed by the EuroQol Group in order to provide a simple, generic measure of health for clinical and economic appraisal. • The EQ-5D-3L descriptive system comprises the following 5 dimensions: mobility, self-care, usual activities pain/discomfort and anxiety/depression. • Each dimension has 3 levels: no problems, some problems, extreme problems. • The respondent is asked to indicate his/her health state by ticking (or placing a cross) in the box against the most appropriate statement in each of the 5 dimensions (Figure1) • EQ-5D-3L descriptive system may be converted into a single summary index by applying a formula that essentially attaches values (also called weights) to each of the levels in each dimension. • HRQoL was calculated using response from EQ-5D using European weights. Table 3. Analysis of HRQoL by fracture Figure 1. EQ-5D survey Conclusions • In a Swedish OP registry, the average HRQoL based on EQ-5D was 0.7. • 34% reported some or extreme problems in mobility; 8% reported some or extreme problems in self-care; 28% reported some or extreme problems in activities; 75% reported some or extreme problems in pain/discomfort; and 43% reported some or extreme problems in anxiety/depression. • Clinical factors that were identified to impact patient reported QoL: • Previous fractures (post age 40), especially in arm, hip and vertebral; Falls during last year; Back pain; Comorbidities (especially asthma, arthritis, and hypertension); Elder age; and Male.






















