Download
1 / 19
210 likes | 403 Views
Experiences and Disorders of the Gynecologic Client Physiology of Puberty, Menarche and Fertility. Marianne F. Moore RN, MSN, CNM. Physiology of Puberty. Puberty refers to the period of sexual maturation.

E N D
Experiences and Disorders of the Gynecologic ClientPhysiology of Puberty, Menarche and Fertility Marianne F. Moore RN, MSN, CNM
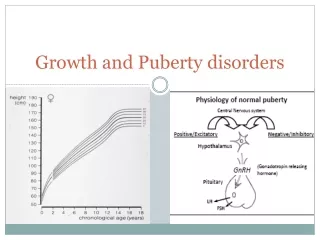
Physiology of Puberty • Puberty refers to the period of sexual maturation. • Puberty is when the child experiences physical, hormonal, and sexual changes and becomes capable of reproduction. • Associated with rapid growth and the appearance of secondary sexual characteristics.
Physiology of Puberty • Changes triggered by hypothalamus and pituitary gland • Ovaries begin to produce estrogen and progesterone • Adolescence is the period of transition between puberty and adulthood.
Physiology of Puberty Before menarche, girls experience • rapid growth, especially an increase in height • breast enlargement • pubic, armpit, and leg hair growth • clear or whitish vaginal secretions • increased hip width
Physiology of Menarche Menarche refers to the starts of the menstrual cycle Occurs between age 9-16 in girls Initial cycles are often anovulatory Irregularity is normal As ovulation established, cycles regulate
Physiology of Menses Follicular Phase • Hypothalamus/GnRH stimulates anterior pituitary to make FSH/LH • FSH causes granulosa cells to make estadiol and follicles are recruited • One follicle dominates and it has the most FSH receptors
Physiology of Menses Follicular Phase • The follicle produces inhibin, and FSH is suppressed • Loss of FSH causes smaller follicles to die off. The dominant follicle grows. • LH causes stromal cells to make androgens close to ovulation-increases sexual desire.
Physiology of Menses Ovulatory phase • Peaking estradiol levels cause a surge of LH and FSH • LH causes resumption of meiosis, luteinization of granulosa cells and progesterone production • 10-12 hours later, the follicular wall breaks down and ovulation occurs
Physiology of Menses Luteal phase • Granulosa and theca cells take up steroids and lutein; corpus luteum. • Progesterone dominated phase • Progesterone suppresses new follicles • Causes secretory changes in the endometrium that support implantation
Physiology of Menses Luteal phase • Progesterone peaks 7-8 days after LH surge; at implantation if it occurs • Luteal phase more constant than follicular phase-14 days if no pregnancy • Progesterone causes the elevation in basal body temperature (BBT) • BBT rise confirms ovulation
Physiology of Menses Menstrual phase • At 9-11 days after ovulation, corpus luteum declines • Progesterone/ estrogen levels decline. • Withdrawal shrinks endometrium, decreases blood flow, and begins pulsatile dilation/constriction of spiral arterioles • Ischemia and stasis alternate with hemorrhage, and menstrual flow begins
Physiology of Menses Menstrual phase • Normal blood loss w/menses 20-80 ml • 70% sloughs by second day • 90% by third day • Average length of menses 4-6 days • Rising estrogen levels by day 5 and thrombin plugs limit blood loss
Physiology of Fertility Female • Estrogen softens cervix and thins mucous; helps sperm to enter uterus • Androgen surge with ovulation increases desire • Oocyte can be fertilized for 12-24 hours after ovulation • Sperm viable in the upper genital tract for up to 72 hours
Physiology of Fertility Female • Cervical mucous favors passage of normal sperm • Improves overall quality of sperm meeting egg • Fertilization occurs in ampullary region of the tube • Fimbria sweep conceptus into uterus • Implantation begins at the blastocyst stage
Physiology of Fertility Male • Male deposits as many as 300 million sperm near cervix with intercourse • Sperm must be normal in shape, adequate in amount and have motility to ascend the genital tract
Physiology of Fertility Male • Some sperm pass through entire tract rapidly; others sit in cervical crypts and ascend later • Sperm are made continuously • Abnormalities can be related to infections, varicoceles, overall health
Cultural considerations • Value of women and children • Role of women in the home and in the world • Menstrual flow as “dirty”
Lifestyle considerations • Personal values • Family needs • Sexual preferences • Personal comfort with own body
Trends in nursing research • Recent research concerns PMS, PMDD and symptom management for menstrual disorders • The Seattle Midlife Women’s Health Study (SMWHS) studied the natural menopausal transition in a population-based sample from 1990 to 2006. • The primary focus of SMWHS throughout the 17 years was on symptoms, hormones, stress and stages of the menopausal transition. • 390 women initially, 176 at end of study