Download
1 / 18
180 likes | 435 Views
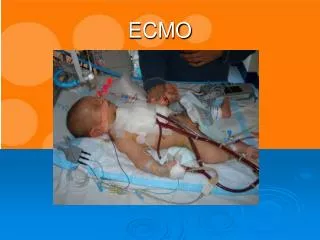
K NDERSPITAL ZÜRICH. PCRRT and ECMO. A. Dodge-Khatami, MD, PhD. University Children‘s Hospital, University of Zürich, Switzerland. D ivision of Congenital Cardiovascular Surgery. K NDERSPITAL ZÜRICH. ECMO. ExtraCorporeal Membrane Oxygenation:

E N D
K NDERSPITAL ZÜRICH PCRRT and ECMO A. Dodge-Khatami, MD, PhD University Children‘s Hospital, University of Zürich, Switzerland Division of Congenital Cardiovascular Surgery
K NDERSPITAL ZÜRICH ECMO • ExtraCorporeal Membrane Oxygenation: • life-saving mechanical circulatory assist device for the temporary support of the cardiac and/or pulmonary systems. • through circulatory support, possibility to maintain homeostasis of all major vital organs, including renal function.
K NDERSPITAL ZÜRICH ECMO • 3 major groups: • respiratory: neonatal & pediatric (82 %) • cardiac: neonatal & pediatric (14.2 %) • adult cardio-respiratory failure (3.8 %)
K NDERSPITAL ZÜRICH Respiratory ECMO • Congenital diaphragmatic hernia • Meconium aspiration syndrome • Respiratory Insufficiency/RDS • Persistent Fetal Circulation/PPHN • Sepsis/Pneumonia • Air leak syndrome
K NDERSPITAL ZÜRICH Respiratory ECMO • indications: • Oxygenation Index (OI)= • mean airway pressure x ([FIO2 x 100]/PaO2) • OI >25 without improvement under ttt or OI >40.
K NDERSPITAL ZÜRICH Respiratory ECMO
K NDERSPITAL ZÜRICH Cardiac ECMO • bridge to myocardial recovery or pre-operative support. • bridge to heart or heart/lung transplantion. • post-operative support after cardiac surgery. • survival to separation from ECMO 53%, and survival to discharge 39%.
K NDERSPITAL ZÜRICH Cardiac ECMO • contraindications?, • relative: age < 35 weeks, weight < 2kg, previous cerebral intraventricular hemorrhage, HLHS + TAPVD. • absolute: profound neurologic deficit or syndrome preventing a meaningful life, against parent will. • as standby: ALCAPA, TAPVD, HLHS
K NDERSPITAL ZÜRICH ECMO
K NDERSPITAL ZÜRICH ECMO neck cannulation if chest closed: right carotid artery + ipsilateral internal jugular vein. confirm lack of need for a vent in the left atrium (possibilty of Rashkind in neonates). post-operative open chest after attemped repair or palliation of congenital heart disease gives direct access to aorta + right atrium + left atrium for left heart decompression.
K NDERSPITAL ZÜRICH ECMO
K NDERSPITAL ZÜRICH ECMO • setup time (15-20 minutes), large priming volume (~300 ml). • maintain ACT 180-220, platelets > 100‘000, fibrinogen > 100 mg/dl, AT III 100%. • when running at lower flows, maximal anticoagulation vs. virtually no anticoagulation when temporarily running at supraphysiologic flows
K NDERSPITAL ZÜRICH ECMO • Cost (CHF): • ECMO system: 1860.- • Blood unit (250 cc) : 218.- • Cannulae (1A + 2V): 810.- • Water prime/rinse: 15.- • Total: 2903.- • Hemofilter: 154.-
K NDERSPITAL ZÜRICH ECMO • duration: • for respiratory ECMO, successful ECMO can be maintained up to ~20 days. • no study has shown survival after 300 hours (12.5 days) for cardiac ECMO; improvement of cardiac function beyond 250 hours is highly unlikely. • when multiorgan failure or sepsis, consider discontinuation after 4 days.
K NDERSPITAL ZÜRICH ECMO complications: mechanical and patient Mechanical: Circuit Clotting (19%) Cannulae placement/flow issues (9%) Air embolism (5%) Oxygenator failure (4%) Connector cracks,pump failure,heat exchanger malfunction (6%)
K NDERSPITAL ZÜRICH ECMO • complications: • Patient • Bleeding (35%) • Ischemic or hemorrhagic cerebral lesions (~15% during, and 40% after decannulation) • Nosocomial infection 30% (risk factor for mortality). • Renal failure (25%): creatinine > 114 µmol/l, urine output < 1 ml/kg/h, or hemofiltration
K NDERSPITAL ZÜRICH ECMO • survival: • >5-fold risk for death in patients requiring hemoflitrationon ECMO as opposed to those who do not (50-65% vs. 9-23%) • „…consideration should be given to discontinueECMO when extrarenal support is required…“ • IS HEMOFILTRATION STARTED TOO LATE, and WOULD EARLIER THERAPY CHANGE PROGNOSIS? • indication for Hemofiltration: volume overload
K NDERSPITAL ZÜRICH ECMO • Hemofilter flow: max 10 ml/kg/hour (zero balance) • Placed BEFORE the oxygenator • Changed once a day • Reduces plasma interleukins (IL-1ra, IL-6, IL-8) induced by cardiopulmonary bypass or ECMO. • No adverse effects on platelet activation and consumption