Download
1 / 28
340 likes | 896 Views
Progressive Supranuclear Palsy and Cortico Basal Degeneration. Presentation for St Johns Hospice Katrina Haines RGN, BSc, MSc kat.haines@pspeur.org- 01995 601533 Nurse Specialist North West and Midlands,

E N D
Progressive Supranuclear Palsy and Cortico Basal Degeneration Presentation for St Johns Hospice Katrina HainesRGN, BSc, MSc kat.haines@pspeur.org- 01995 601533 Nurse Specialist North West and Midlands, North Wales, Northern Ireland and Republic of Ireland
PSP and CBD Introduction to PSP/CBD: • pathology, • types, • stages, • symptoms • disease management
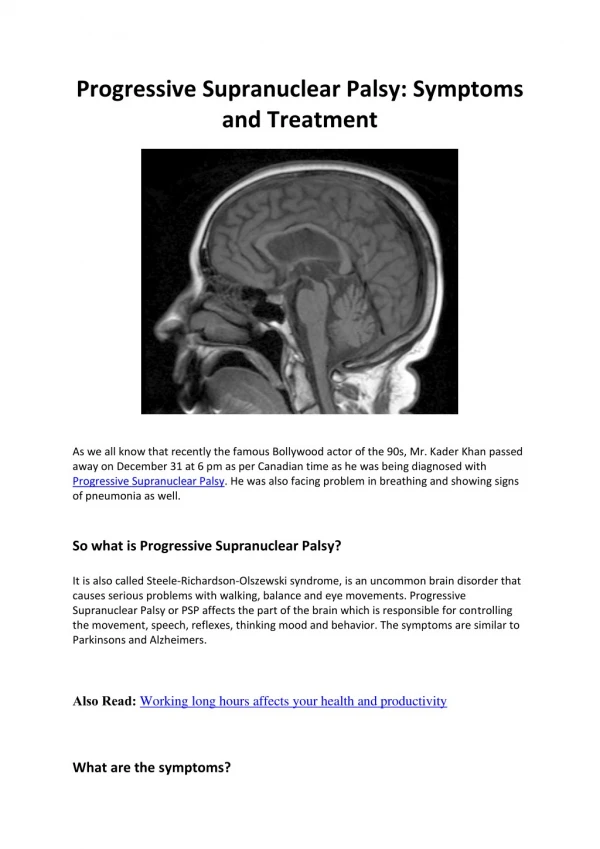
Overview of Progressive Supranuclear Palsy (PSP) • What is PSP?Also known as Steele Richardson Olszewski syndrome Chronic, terminal neuro-degenerative disorder Degeneration of brainstem structures • What is the patient population?Prevalence - 6.4 per 100,000 (may be higher)-MND • Adult onset (mid 50s - mid 70s) Patients usually die within 5/10 yrs -onset of symptoms and 2/4 years from diagnosis • What are the symptoms?Disturbance of balance • Impaired mobility • Disordered vertical gaze • Progressive disorder of speech and swallowing 1
PSP - Symptoms • Postural Instability • Eye Problems • Swallow Problems • Speech Problems • Cognitive Changes • Bladder and Bowel • Pain
CBD – What is it? • Numbness, jerking fingers, loss of use of one hand • Asymmetric; progressively affecting arm and leg • Alien limb • Less common disturbance of eye movement • Increased frontal lobe deficit Cortico Basal Degeneration – similar to PSP except:
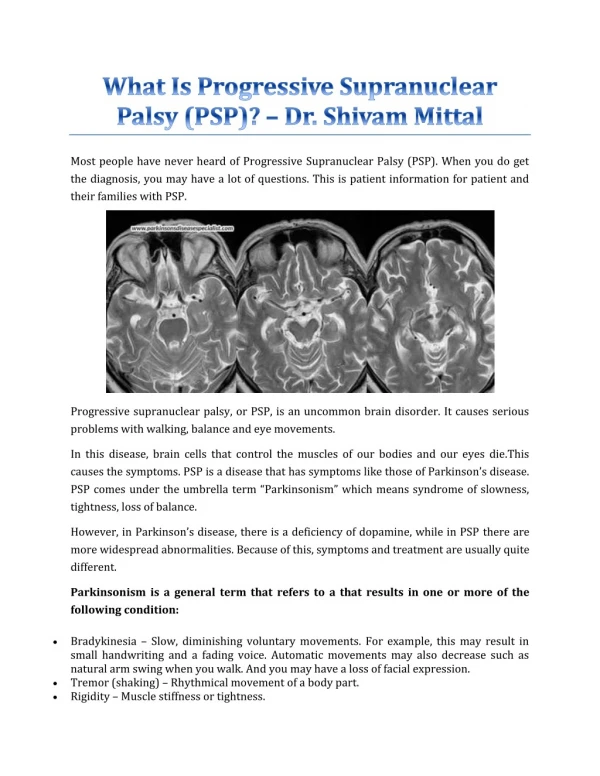
Mid brain atrophy • Neuronal loss4 • Neurofibrillary tangles in the basal ganglia, diencephalon and brainstem4 Minimal cortical pathologyexcept for motor areas4 Some cases of PSP map to a polymorphism in the tau gene4 Pathology of PSP
PSP – Differential Diagnosis • Poor levodopa response (compared to PD) • No presenting tremor • Usually affects people over 40 • Falls are often backwards • Steady deterioration • Restricted eye movement • Neurofibrillary tangles not Lewy Bodies
PSP/CBD is relentlessly progressive It is now recognised that some forms of PSP follow a more benign course. The proximate cause of death in many cases is aspiration pneumonia. Median interval (yrs) from initial symptom to development of major deficits (Golbe 1988) Initial gait difficulty 0.3 Aid needed to walk 3.1 Dysarthria 3.4 Visual symptoms 3.9 Dysphagia 4.4 Confined to bed or wheelchair 8.2 Death 9.7 Natural history of PSP
PSP types Richardson Syndrome( most common) • Postural instability and Falls • Cognitive dysfunction • Bulbar signs • Supranuclear gaze palsy/Abnormal saccades PSP-Parkinsonism( less severe) • Bradykinesia/tremor • Limb dystonia • Asymmetric onset • Levodopa responsive rigidity Pure Akinesia with Gait Freezing • Early falls and movement difficulties • Late bulbar problems • Rarely eye problems • No dementia
Posture Increased stiffness Nunchal rigidity-coat hanger pain refers into arms or head Head pokes forward at the chin or chin in the air- retrocollis Thoracic spine -axial rigidity or kyphosed if slumped Pelvic area becomes stiff
PSP – Postural Instability PROBLEMS • Falls - often backwards • Difficulty with down gaze, shuffling, broad based gait • Stiff arched neck, axial rigidity • Tiredness, light-headedness • Sudden change of direction, loss of balance • Sitting “en bloc” “rocket sign” make stairlifts difficult MANAGEMENT • O.T. – grab rails, ramps, through floor lift, adaptations to home, equipment • Helmet and hip protectors • Limited benefit from PD drugs
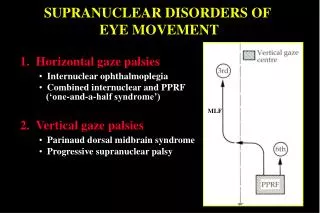
PSP - Eye Problems • Problem with movement of the eye itself • Starts with slow saccades • Later limited voluntary vertical saccades • Especially down gaze • Reflex movements remain normal (Doll’s eye manoeuvre) • Indicating supranuclear problem fault with eye muscle innervation not eye muscles • Upper motor neuron paresis • Limited up gaze can be normal in elderly but never accompanied by slow saccades
Management of Eye Lid Problems • Position in sight line • Prism glasses • Ptosis props or tape • Eye drops, Artificial tears (clarymist spray) • Tinted wrap around glasses • Botox injections • Educate / Awareness family
PSP – Swallow Problems PROBLEMS • Eat too quickly • Overfill Mouth • Weak cough / choke • Excess salivation • Aspiration pneumonia MANAGEMENT • Early referral to speech therapist • Dietician – supplements • Swallowing techniques • Softened diet / thickened fluids • Videofluoroscopy • PEG insertion
PSP – Speech Problems PROBLEMS • Delay in response, word search • Reduced facial expression • Palalalia, stuttering • Three types of speech pattern: • Hypokinetic Dysarthria – like PD, quiet, repetition of sounds • Spastic Dysarthria – strained, slow and slurred • Ataxic Dysarthria – slurred and imprecise, sounding drunk MANAGEMENT • Early involvement of Speech and Language Therapist • Exercises for speech-singing • Communication aids: Picture and alphabet boards, amplifiers, electronic aids
PSP – Cognitive Change PROBLEMS • Intelligence largely intact • Loss of higher executive function • Sleep disturbance • Short term memory problems • Impaired judgement or reasoning • Irritability, aggression, apathy • Emotional lability • Depression, general lack of interest • Vague changes in personality MANAGEMENT • Need for families to understand • Support for families, recognising emotions • Antidepressant drugs
PSP - Pain COMMON PAINS • Check with GP for any underlying cause • Neck (and referred) • U.T.I • Cramp as stiffness increases • Possible contractures • General aches from postural and muscle weakness MANAGEMENT • Passive Exercises • Postural management • Warmth, analgesia • Muscle relaxants • Massage • Complementary therapies, acupuncture, reflexology, aromatherapy, exercise for as long as possible
PSP – Bladder & Bowel Problems PROBLEMS • Difficulty with initiating flow • Oversensitivity • Nocturnal Enuresis • U.T.I • Incontinence • Constipation • Loss of bowel control MANAGEMENT • Increase fluids • Increase fruit and roughage in diet • Continence advice nurse • Bottle, commode • Pads, sheath • Catheter – either intermittent or permanent • Suppositories and enemas
Palliative Care • Incurable deteriorating condition-QoL • Support from diagnosis-all aspects of living • GP Palliative care register • MDT management -identified care co-ordinator • Proactive monitoring of changes and symptom management. • Continuing health care funding • Access to respite / hospice care • Anticipatory care planning/Advanced decisions • Care and support for carers
DRIVERS • Long term neurological conditions NSF • Living matters dying matters 2010 • National Council for Palliative Care 2006 • World Health Organisation 2005 • Gold Standards Framework • Liverpool Care Pathway • Mental Capacity Act 2005
Drug Treatment for PSP No specific licensed treatment Anti-parkinsonian drugs – modest benefit, may cause side effects2,3 Amantadine – may benefit some patients3 Botulinum toxin –for neck muscle spasm and blepharospasm3 Artificial tears–for dry eyes9 Antidepressants –(amitriptyline helpful for sleep disturbance) Excessive salivation -glycopyrronium/atropine
CHALLENGES OF PSP • MEDICAL MANAGEMENT • CO-MORBIDITIES • INDIVIDUAL VARIABILITY OF CONDITION • DETERMINING END OF LIFE
PSP – Nurse Specialists Helpline Talks/Study sessions Support Groups 30 around the UK and RoI Including Lancaster, Manchester, Holmes Chapel • Clinics • London • Coventry • Cambridge • Newcastle • Newport • Manchester • Brighton • Edinburgh