Download
1 / 1
10 likes | 133 Views
“When Was Your Last Drink?” – A Prenatal Screening in Brazzaville Andrew D. Williams, MPH 1,3 ; Yannick Nkombo 2 ; Gery Nkodia 2 ; Larry Burd, PhD 1 ; Chunzi Peng , PhD 1 North Dakota Fetal Alcohol Syndrome Center, University of North Dakota, Grand Forks, ND

E N D
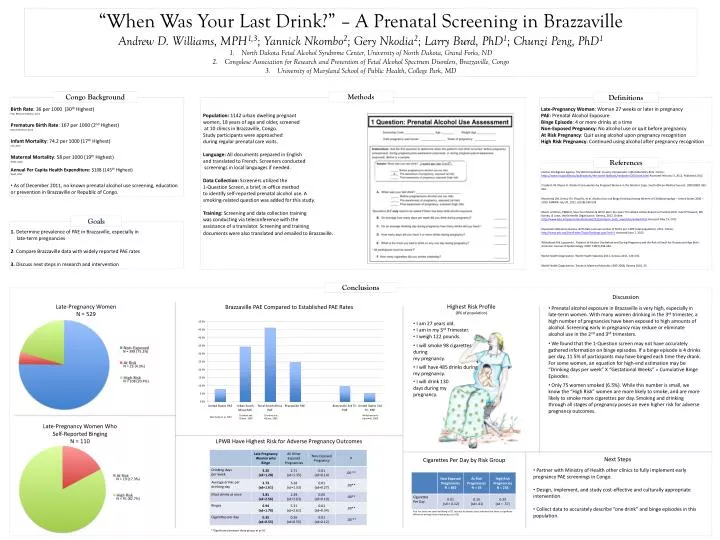
“When Was Your Last Drink?” – A Prenatal Screening in Brazzaville Andrew D. Williams, MPH1,3; Yannick Nkombo2; Gery Nkodia2; Larry Burd, PhD1; ChunziPeng, PhD1 North Dakota Fetal Alcohol Syndrome Center, University of North Dakota, Grand Forks, ND Congolese Association for Research and Prevention of Fetal Alcohol Spectrum Disorders, Brazzaville, Congo University of Maryland School of Public Health, College Park, MD Methods Congo Background Definitions • Birth Rate: 36 per 1000 (30th Highest) • Pop. Reference Bureau, 2011 • Premature Birth Rate: 167 per 1000 (2nd Highest) • March of Dimes, 2012 • Infant Mortality: 74.2 per 1000 (17th Highest) • CIA, 2012 • Maternal Mortality: 58 per 1000 (19th Highest) • WHO, 2010 • Annual Per Capita Health Expenditure: $108 (145th Highest) • WHO, 2011 • As of December 2011, no known prenatal alcohol use screening, education or prevention in Brazzaville or Republic of Congo. Population: 1142 urban dwelling pregnant women, 18 years of age and older, screened at 10 clinics in Brazzaville, Congo. Study participants were approached during regular prenatal care visits. Language: All documents prepared in English and translated to French. Screeners conducted screenings in local languages if needed. Data Collection: Screeners utilized the 1-Question Screen, a brief, in-office method to identify self-reported prenatal alcohol use. A smoking-related question was added for this study. Training: Screening and data collection training was conducting via teleconference with the assistance of a translator. Screening and training documents were also translated and emailed to Brazzaville. Late-Pregnancy Woman: Woman 27 weeks or later in pregnancy PAE: Prenatal Alcohol Exposure Binge Episode: 4 or more drinks at a time Non-Exposed Pregnancy: No alcohol use or quit before pregnancy At Risk Pregnancy: Quit using alcohol upon pregnancy recognition High Risk Pregnancy: Continued using alcohol after pregnancy recognition References Central Intelligence Agency. The World Factbook: Country Comparison: Infant Mortality Rate. Online: https://www.cia.gov/library/publications/the-world-factbook/rankorder/2091rank.html Accessed February 3, 2012. Published 2012. Croxford J & Viljoen D. Alcohol Consumption by Pregnant Women in the Western Cape. South African Medical Journal. 1999 (89)9; 962-962. Marchetta CM, Denny CH, Floyd RL, et al. Alcohol Use and Binge Drinking Among Women of Childbearing Age – United States 2006 – 2010. MMWR. July 20, 2012. 61(28);534-538. March of Dimes, PMNCH, Save the Children & WHO. Born Too Soon: The Global Action Report on Preterm Birth. Eds CP Howson, MV Kinney, JE Lawn. World Health Organization. Geneva, 2012. Online: http://www.who.int/pmnch/media/news/2012/preterm_birth_report/en/index4.html Accessed May 15, 2012. Population Reference Bureau. Birth Rate (annual number of births per 1,000 total population). 2011. Online: http://www.prb.org/DataFinder/Topic/Rankings.aspx?ind=3. Accessed June 7, 2012. Whitehead N & Lipscomb L. Patterns of Alcohol Use Before and During Pregnancy and the Risk of Small-for-Gestational-Age Birth. American Journal of Epidemiology. 2003. 158(7);654-662. World Health Organization, World Health Statistics 2011, Geneva 2011, 128-135. World Health Organization, Trends in Maternal Mortality 1990-2008, Geneva 2010, 23. Goals 1. Determine prevalence of PAE in Brazzaville, especially in late-term pregnancies 2. Compare Brazzaville data with widely reported PAE rates 3. Discuss next steps in research and intervention Conclusions Discussion Late-Pregnancy Women N = 529 Highest Risk Profile (8% of population) Brazzaville PAE Compared to Established PAE Rates • Prenatal alcohol exposure in Brazzaville is very high, especially in late-term women. With many women drinking in the 3rd trimester, a high number of pregnancies have been exposed to high amounts of alcohol. Screening early in pregnancy may reduce or eliminate alcohol use in the 2nd and 3rd trimesters. • We found that the 1-Question screen may not have accurately gathered information on binge episodes. If a binge episode is 4 drinks per day, 11.5% of participants may have binged each time they drank. For some women, an equation for high-end estimation may be “Drinking days per week” X “Gestational Weeks” = Cumulative Binge Episodes. • Only 75 women smoked (6.5%). While this number is small, we know the “High Risk” women are more likely to smoke, and are more likely to smoke more cigarettes per day. Smoking and drinking through all stages of pregnancy poses an even higher risk for adverse pregnancy outcomes. N = 398 (75.2%) N = 19 (17.3%) • I am 27 years old. • I am in my 3rd Trimester. • I weigh 122 pounds. N = 23 (4.3%) N = 91 (82.7%) N = 108 (20.4%) • I will smoke 98 cigarettes during • my pregnancy. • I will have 485 drinks during my pregnancy. Late-Pregnancy Women Who Self-Reported Binging N = 110 • I will drink 130 days during my pregnancy. Croxford and Viljoen, 1999 Croxford and Viljoen, 1999 Whitehead and Lipscomb, 2003 Marchetta et al, 2012 LPWB Have Highest Risk for Adverse Pregnancy Outcomes Next Steps Cigarettes Per Day by Risk Group • Partner with Ministry of Health other clinics to fully implement early pregnancy PAE screenings in Congo. • Design, implement, and study cost-effective and culturally appropriate intervention. • Collect data to accurately describe “one drink” and binge episodes in this population. Post hoc tests (we used Hochberg’s GT2 test due to sample sizes) indicated that there is significant difference among these three groups. (p<.05). **Significance between these groups at p<.01