Download

1 / 23
230 likes | 328 Views
Effect of Socioeconomic Status on Cardiovascular Care. “Reverse Targeting”. Professor Shahryar A. Sheikh President, World Heart Federation 1 st Annual Dr. Abdul Haque Khan Memorial International Cardiology Symposium Karachi 14 March 2008. Advance Cardiac Care. 80%. 3 %. 11 %. 16 %.

E N D
Effect of Socioeconomic Status on Cardiovascular Care “Reverse Targeting” Professor Shahryar A. Sheikh President, World Heart Federation 1st Annual Dr. Abdul Haque Khan Memorial International Cardiology Symposium Karachi 14 March 2008
Advance Cardiac Care 80%
3 % 11 % 16 % 26 % 15 % Turkey 71 % 19 % Mexico Poland Spain 39 % Japan OECD avg. Distribution of Global Population & Health Expenditure, by Income in 2000 Italy Greece France Germany United States % GDP to Health Population, % Health $, PPP, % ■ High, >$16,000 ■Higher Middle, $ 6-16000 ■Lower Middle, $ 2 - 6000 ■ Low, <2000 Globalization Research Centre, 2004;1:10
Cardiac Surgical Procedures Performed on an Annual Basis Globally Worldwide Survey on Cardiac Interventions, 1995 Number of Cases The Number of cardiac surgical procedures performed on an annual basis globally (Reproduced from Unger F. Worldwide survey on cardiac intervention 1995. Cor European 1999;7:128-46: with permission of Springer-Verlag) Unger F, Cor Europpaeum. 1999;7:128-46
Indonesia Brazil India Kenya Inequalities in health between and within countries: poverty and inequality Under-5 mortality rates per 1000 live births by socioeconomic quintile of household
Death rates from CHD by socio-economic class, age 15 or 20 to 74 years, England and Wales Deaths per 100,000 250 Professional 200 Intermediate N Skilled non-manual 150 M Skilled manual 100 Partly skilled 50 Unskilled 0 1970/72 1990/93 Drever et al Pop. Trends 1996;86:15-20
SOCIAL INEQUALITIES IN MALE MORTALITY IN FROM SMOKING AND FROM ANY CAUSE (1996) USA Canada Poland England and Wales 50% 50 Smoking Any Cause 43% 40 37% 36% 34% 32% 31% 30 26% 24% 22% 21% Riskof dying at ages 35-69 years (%) 21% 20% 19% 20 15% 14% 13% 10% 10% 10 8% 6% 5% 4% 4% 0 Low (V) High (I/II) Med (III/IV) Med (60%) Low (20%) High (20%) Med (12 yrs) Med (12 yrs) Low (<12 yrs) Low (<12 yrs) High (>12 yrs) High (>12 yrs) Social class Education Neighborhood Income Education P Jha et al., Lancet 2006; 368:367
Selected Health Status Indicators: National Health Survey of Pakistan, 1990–1994 G. Pappas, W.C. Hadden, T. Akhtar, A J of Public Health 2001;91:93-98
Selected Health Status Indicators Comparing the United States and Pakistan: National Health Survey of Pakistan, 1990–1994, and NHANES III, 1988–1994 G. Pappas, W.C. Hadden, T. Akhtar, A J of Public Health 2001;91:93-98
Indicators of Access to and Appropriateness of Health Care for Adults National Health Survey of Pakistan, 1990–1994, and NHANES III, 1988–1994 G. Pappas, W.C. Hadden, T. Akhtar, A J of Public Health 2001;91:93-98
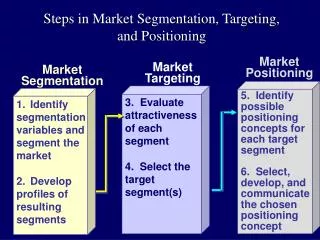
Men Overall Rates Percent Percent Income Quartile Women Percent Income Quartile Income Effects of Socioeconomic Status on PCI & CABG Alberta, Canada Am. J M, 2007, 120, 33-39
Socioeconomic Status Access to Cardiac Procedures and Mortality Rates of Use of Procedures and Waiting Times Ratio Income Quintile Adjusted Relative Rates of Angiography within Six Months after Acute Myocardial Infarction, Waiting Times for Angiography, and One-Year Mortality According to Income Quintile.
Socioeconomic Status Access to Cardiac Procedures and Mortality Days after Acute Myocardial Infarction Kaplan-Meier Survival Curves According to Quintile of Neighborhood Median Income David A. alter.,NEJM 1999;341:1359-67
21 % 8 % 8 % 60 % 10 % 7 % 9 % 77 % 16 % 13 % 64 % 7 % Cardiovascular Care in Pakistan Out Patients (2006) In Patients (2006) Total PCI 1886 ■ Paying■Poor ■G. User ■Entitled S. Sheikh, ESC, 2007
In Patients PTMC 21 % 6% 3 % 60 % 6 % 10 % 9 % PCI 85 % 16 % 13 % 64 % 7 % Socioeconomic Status and Cardiovascular Disease ■ Paying■Poor ■G. User ■Entitled S. Sheikh, ESC, 2007
Socioeconomic Gradient and Cardiovascular Care 39% 9% 22% 11% S. Sheikh, ESC, 2007
The World’s Priorities? Annual Expenditure *Estimated additional annual cost to achieve universal access to basic social services in all developing countries Human development Report 1998
Expanding gap between the wealthy and the poor in our society represents the single greatest threat to our free standing democracy. SENATOR BOB KERY (Nebraska)
No other group of people in world can claim such a wonderful position in life or more rewarding job. Because of our unique talent and position in world’s social spectrum. We have social obligations that only we are capable of addressing. Let us light a candle instead of deploring the darkness.
Socioeconomic gradient remains the most important barrier amongst the countries, or within a developing country, for appropriate application of cardiovascular care.
Next World Congresses: • 2008 World Congress of Cardiology, Buenos Aires,Argentina - http://www.worldcardiocongress.org • 2010 World Congress of Cardiology, Beijing, China Sharing Science/Building Capacity