Download
1 / 36
820 likes | 2.08k Views
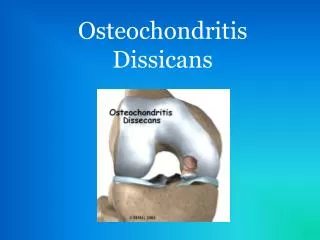
Osteochondritis Dissecans of the Knee. Tim Francisco Orthopedics Topic. Osteochondritis Dissecans. Definition: Idiopathic Lesion of subchondral bone that becomes necrotic.

E N D
Osteochondritis Dissecansof the Knee Tim Francisco Orthopedics Topic
Osteochondritis Dissecans • Definition: • Idiopathic Lesion of subchondral bone that becomes necrotic. • With motion and lack of underlying support, the cartilage may degenerate and eventually a focal area of subchondral bone (with or without articular cartilage) will separate from adjacent bone
Incidence 30-60/100,000 10-20 years of age can occur up through 50 years of age Male/Female-3:1 Right knee>Left knee Bilateral 30% 2 Types Juvenile (JOCD) before epiphyseal closure Adult (ACOD or OCD) closed physes Osteochondritis Dissecans
1854: Broca postulated that spontaneous necrosis and subsequent mobilization of fragments accounted for loose bodies 1870: Paget agreed and described OCD in the knee OCD: History
OCD: History • 1887: König provided the term, osteochondritis dissecans • described trauma to articular surface leading to necrosis and then zone of “dissection inflammation • No histologic evidence for an inflammatory component
1 Exogenous Trauma 2 Endogenous Trauma 3 Ischemia 4 Abnormal ossification 5 Genetic 6 Combination OCD: Etiology Many etiologies have been proposed and investigated.
OCD: Etiology • Trauma likely a key factor, especially in JOCD • 40% relate Hx of mild to moderate knee trauma • Cyclic or repetitive trauma • 1976 Linden reports incidence related to popularity of sports • 1975 Cahil notes average age from 12.9 to 11.3 years with in females with JOCD. He also relates this earlier participation in organized sports
OCD: Clinical Presentation • Vague symptoms of low grade knee pain • Usually of several months duration • related to level of physical activity • No acute trauma but possible past Hx of trauma • Swelling, locking, crepitus may be present
Exam may be normal Joint effusion Crepitus Painful joint motion Palpable loose body Localized pain to palpation at the lesion medial femoral condyle Common finding of thigh atrophy OCD: Physical Exam
OCD: Physical Exam • Wilson’s test (Positive for lesions in classic site) • Patient seated with 90° knee flexion • examiner internally rotates tibia then extends knee • Patient experiences pain at 30° of flexion • External rotation of tibia relieves pain • Anterior tibial spine impacts on the medial femoral condyle
OCD: Differential DX • Meniscal tears • Osteochondral Fracture • Osteonecrosis • DJD • Multiple epiphyseal dysplasia
OCD: Diagnostic Studies • Radiographic examination diagnostic • AP • Lateral • Patellofemoral • Tunnel view most important
Insert xrays here A/P View
OCD: Diagnostic Studies • MRI • Assess articular cartilage integrity • Assess lesion stability • less useful for identifying loose bodies
T1 weighted coronal T1 weighted sagittal
OCD: Diagnostic Studies • Bone Scintigraphy • prognostic indicator • Monitor lesion healing with serial scans • Classification schemes
OCD: Diagnostic Studies • Arthroscopy • Definitive assessment of lesion stability and articular cartilage integrity • Identification of loose bodies • Classification Schemes • Treatment
OCD: Classification • MRI • 1. Junction of fragment and underlying bone • 2. Discreet, round homogeneous area deep to lesion • 3. Focal defect in articular cartilage • 4. Line traversing cartilage and subchondral bone
OCD: Classification • Bone Scintigraphy Stages I-IV have abnormal radiographs • Stage 0 Normal knee • Stage I normal bone scan poor • Stage II isotope uptake • Stage III isotope uptake in lesion and femoral condyle • Stage IV isotope uptake in adjacent tibial plateau
OCD: Classification • Arthroscopic appearance • Type I intact articular surfaces, not mobile • Type II early separation, intact articular cartilage but fragment mobile • Type III disrupted articular surface • Type IV crater with loose or fragmented lesion
Partially detached lesion Elevation of lesion demonstrating the crater
OCD: Prognosis • JOCD: generally good prognosis • 50% spontaneously heal within 10-18 months • compliant patient, stable lesion, not near age of physeal closure • AOCD or OCD: worse prognosis with physeal closure • Linden reported 80% of patients showed evidence of DJD 10 years earlier than matched controls • included all 3 compartments • many had loose bodies
OCD: Treatment • Treatment based on • lesion size, stability, symptoms, skeletal maturity • Goals • eliminate symptoms • restore joint surface • healing of fragment • avoiding long term degenerative changes
OCD: Treatment • Nonsurgical indications • All JOCD except for loose or detached bodies • Not much role for AOCD, even with stable fragment. • Trial of conservative treatment? • Compliance is necessary
OCD: Treatment (non-surgical) • 10-12 weeks • Relative rest with or without protective weight bearing • Immobilization should be avoided b/c of detriment to articular cartilage • Decrease activity to achieve pain free status
Indications Failed conservative treatment unstable lesions detached lesions skeletal maturity Goals Enhance vascularization of fragment to encourage union reduction for anatomic restoration of joint surface enhance revascularization of replaced fragment to promote union OCD: Treatment (surgical)
Removal of loose bodies Every attempt should be made to replace the fragment especially on weight bearing surfaces long term results of fragment removal poor Preparation of fragment and base of lesion is essential curette fibrous tissue drill subchondral bone crater add cancellous bone graft if surface not congruous OCD: Treatment (surgical)
Drilling K wire Bone peg fixation Pin fixation Cannulated screw Herbert screw Retrograde bone grafting Fragment removal with drilling and abrasion Osteochondral allografts OCD: Treatment (surgical)
OCD: Summary • Early recognition • Staging of lesion as to stability, size, skeletal maturity to determine treatment plans • Follow-up to monitor healing • Goals • eliminate symptoms • restore joint surface • healing of fragment • avoiding long term degenerative changes