Download
1 / 51
560 likes | 833 Views
Diagnosis, Staging, and Grading of Breast Cancer. Francis Ikpatt. Breast profile: A ducts, B lobules, C dilated section of duct to hold milk D nipple, E fat, F pectoralis major muscle, G chest wall/rib cage Enlargement:

E N D
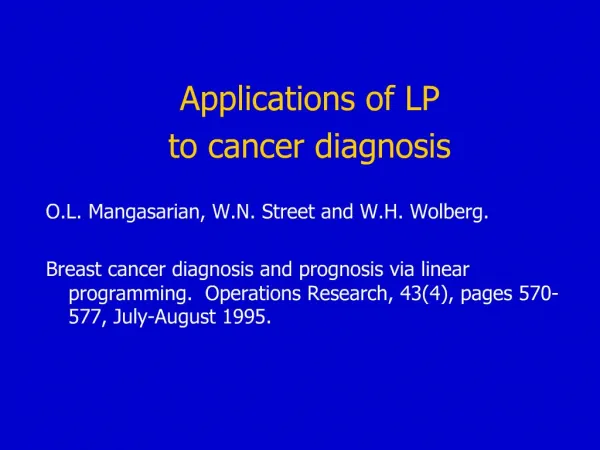
Diagnosis, Staging, and Grading of Breast Cancer Francis Ikpatt
Breast profile: A ducts, B lobules, C dilated section of duct to hold milk D nipple, E fat, F pectoralis major muscle, G chest wall/rib cage Enlargement: A normal duct cells, B ductal cancer cells breaking through the basement membrane C basement membrane
Breast profile: A ducts, B lobules, C dilated section of duct to hold milk D nipple, E fat, F pectoralis major muscle, G chest wall/rib cage Enlargement: A normal duct cells, B ductal cancer cells breaking through the basement membrane C basement membrane .
Breast Self Examination can pick up suspicious lumps and nipple discharges Start BSE at 20 years and encourage self awareness
Active cells, which often indicate rapid cancer growth, take up the radioactive material. This helps radiologists identify areas where cells are suspiciously active, which can indicate cancer
SENTINEL LYMPH NODE DISSECTION remove only the one node that is most likely to have it. If this node is clean, chances are the other nodes have not been affected. In reality, the surgeon usually removes a cluster of two or three nodes—the sentinel node and those closest to it.
Lymph Node Areas Adjacent to Breast Area A Pectoralis major muscleB Axillary LN: levels IC AxillaryLN: levels IID Axillary LN: levels IIIE Supraclavicular LNF Internal mammary LN
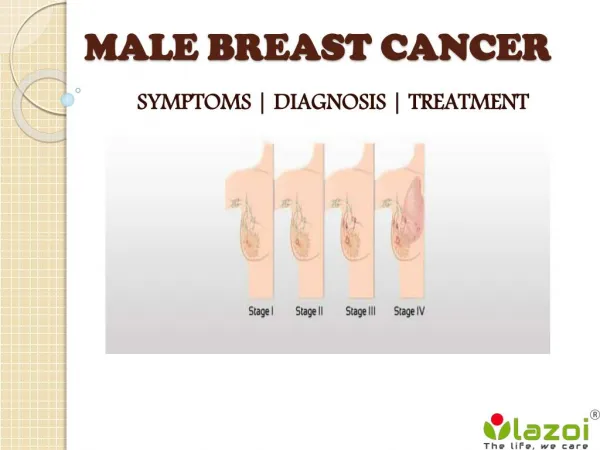
Stage IIIA is defined as T0 - T3 N2 M0 or T3 N1 M0. Stage IIIB is defined as T4 any N M0 or any T N3 M0.
Other Diagnostic Techniques • Tumor markers CA 15.3, CA125, CA 27.29 (early indicator of disease progression or recurrence) • Chest X-Ray -Spread to lungs and heart -Assess lungs before anaesthesia and chemotherapy -Assess infections and radiation induced pneumonia • Bone scintigraphy(bone scan) -detect the presence of bone metastases -evaluate persistent or progressive bone pain -different from a bone density study (DEXA scan is the most popular type), which evaluates bone strength and your risk of osteoporosis -not necessary for DCIS
Ductal Lavage - suction is applied to the nipple to bring out fluid from the many little milk ducts that end in the nipple. • small canula, or tiny tube, is placed into the milk duct, and then fluid is washed into the duct to rinse out cells. • This fluid is then pulled back out of the nipple and sent to the laboratory for evaluation under the microscope. Some call this technique a "Pap smear" of the breast.
Sestamibi complements mammography—it will not replace it. • Sestamibi also called Miraluma are using to detect active breast cancer cells, in the breast and in other parts of the body • Injection of a radioactive substance called technetium 99. This substance, which emits low levels of radiation, gets picked up by tumors, so radiologists can see the tumors on film • Sestamibi does not detect calcification
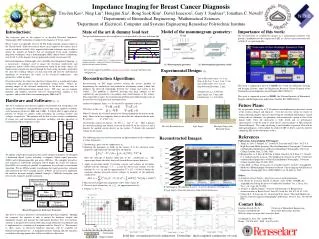
Assess mean nuclear area (mna), mitotic index (smi),fraction of fields with tubular differentiation (ftd) in BC from African-Americans (AA-166) Caucasians (C-170) Nigerians (N-148)
Biomarkers of human breast cancer ER Ki67 CD34 HER2+ P53
Upper panel. Breast tissue microarray containing representative samples of the whole spectrum of breast pathology in a single slide. Lower Panel. A. Tissue microarray sample of an invasive ductal carcinoma of the breast stained with hematoxylin and eosin. B. Same tumor staining positive for RhoC overexpression with a polyclonal anti-RhoC antibody
tumor size mean 4.2±1.3cm mean age 43.8±11.2 years 66.9% are premenopausal 73% are advanced (stages III and IV)
This wheel of tumor characteristics is used to prognosticate individual patients' chances of recurrence
Patients’ Bill of Right • A diagnosis within a week of a suspicious mammogram and biopsy. You'll want a quick diagnosis to allay your anxiety. • A prompt referral by your family doctor to a breast specialist or team specializing in breast cancer • A breast specialist with whom you feel comfortable • A specific diagnosis. You know you have breast cancer, but you need to know its attributes • A second opinion • A copy of medical records, including your pathology report
Patients’ Bill of Right • Information about your condition and treatment options in language you understand • Know the scientific evidence behind your doctor's treatment recommendation, and the strength of that evidence • Information about the benefits and risks of a particular treatment in your case-including the benefits and risks of not having the treatment. • A referral to another breast specialist if you're having trouble communicating with your doctor.
Pathologists In Medical Malpractice Cases • Pathologists are responsible for making or confirming the diagnosis of cancer • malpractice often involves cancer diagnosis • Misdiagnosing a benign condition as cancer can subject a patient to debilitating tx and the emotional trauma of a death sentence • Misdiagnosing cancer as a benign condition can result in delay in diagnosis, allowing a curable cancer to become incurable.
Medical Malpractice and Breast Cancer • Too many women have their breast cancer diagnosis delayed when the physician and other health care providers in whose hands such women entrust their well-being fail to • perform appropriate screening tests • properly interpret test results • take necessary steps when bc is suspected • when this happens, the physician or other health care provider are negligent. • the tragic result of this negligence is too often the loss of treatment options and/or the loss of chance of survival.
Failure to diagnose breast cancer • 40 percent of all medical malpractice suits filed in 1999. • Several of the top ten lawsuits settled (over 1 million dollars) in Massachusetts involved medical malpractice where a physician failed to identify, in a timely manner, a serious case of breast cancer. • is a form of medical malpractice, which is the negligent or incorrect performance of the professional duties of health care providers and institutions. • there are four prerequisites for a valid claim of medical malpractice:1) A provider-patient relationship existed; 2) Negligent care was rendered; 3) the patient suffered damage or harm; 4) and the damage or harm done to the patient was a direct result of the negligent care.
Reasons why doctors misdiagnose breast cancer. • relying too much on a woman's age as a predicting factor for breast cancer. • relying too heavily on negative mammogram results, even if the woman has felt a lump. • don't take woman seriously when they complain of symptoms.