Download
1 / 24
330 likes | 519 Views
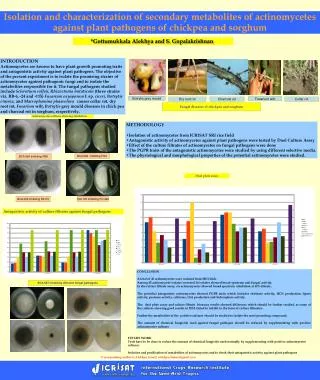
ACTINOMYCETES & NOCARDIA. Dr Sathya Anandam. ACTINOMYCETES. Gram positve , non motile, non sporing , non capsulated filamentous bacteria Thin bacteria with muramic acid cell wall. Superficial resemblance to fungi due to branching filaments.

E N D
ACTINOMYCETES & NOCARDIA Dr Sathya Anandam
ACTINOMYCETES • Gram positve, non motile, non sporing, non capsulated filamentous bacteria • Thin bacteria with muramic acid cell wall. • Superficial resemblance to fungi due to branching filaments. • Related to Corynebacteria and mycobacteria
Includes genera: - Actinomyces, Arachnia, Bifidobacterium - Nocardia, Actinomadura, Streptomyces
ACTINOMYCES • Soil saprophytes & commensals of oral cavity • Cause actinomycosis - a chronic granulomatous disease • Indurated swelling, suppuration and discharging of sulfur granules from sinuses. • Later stage leads to fibrosis & tissue destruction • Infection usually endogenous. • A.israelli is the MC cause.
The name refers to ray – like appearance of the organism in the granules( Actinomyces, meaning ray fungus) • Mode of infection: mostly endogenous & trauma e.g. dental extraction
Worldwide in distribution More common in rural areas and agricultural workers Young males 10-30 yrs age group more common. Pelvic infection seen in women using intrauterine devices. Organism occurs as commensal in mouth, URT and female genital tract. Have low virulence
Pathogenesis • Enters the tissue, and bridges the mucosal or epithelial surface • Creates an anaerobic environment • Induces mixed inflammatory response • Forms painless indurated swelling with sinuses which may drain pus containing granules to the skin surface • Infection spreads to neighbouring organs with bone destruction
Clinical manifestations • 4 clinical forms; 1. cervicofacial- lumpy jaw 2. Thoracic 3. Abdominal 4. Pelvic • Disseminated form- hematogenous spread • Also associated with inflammatory disease of gums. • Can also present as mycetoma • The disease is characterised by presence of Sulfur granules in the exudate
Laboratory diagnosis • Specimen- pus, sputum, BAL,biopsy • Gross examination of granules • Microscopy: pus discharge is washed thoroughly in saline in a test tube • Sediment is collected which is crushed between two slides and smears are made
Gram’s staining: shows a central mass of Gram positive filamentous bacilli, radiating peripherally with hyaline, club- shaped ends • Granules are hard and non emulsifiable • Fluorescent antibody techniques • Fluorescent in situ hybridization
Histopathological staining: H & E stain/ Gomori’s stain on tissue sections reveal • Granules composed of eosinophilic clubs surrounding basophilic filaments and inflammatory cells such as neutrophils & macrophages- sun ray appearance
Sulfur granules are white to yellow with siz ranging from minute specks to about 5mm and are found only in tissue.
Isolation in culture- granules are washed and cultured anaerobically at 370C on BHIA and Thioglycollate broth. • A. israelli- small spidery colonies which become heaped up, white irregular or smooth and large in 10 days, on thioglycollate btoth fluffy balls at the bottom of tube • Species identification
TREATMENT • MEDICAL TREATMENT- prolonged treatment with penicillin or tetracycline for 6-12 months to prevent relapse • SURGICAL TREATMENT- drainage or excision
NOCARDIA • Gram positive branching filamentous bacilli • Aerobic and acid fast • PRESENT IN SOIL • Infection exogenous • Species associated N.asteroides, N. Brasiliensis and N. caviae
Pathogenesis • Worldwide, common in adult males • Inhalation of fragmented bacterial mycelia- pulmonary nocardia • Transcutaneous inoculation of bacteria- cutaneous/ sub cutaneous e.g mycetoma • Characteristic histological feature is an abscess with extensive neutrophilic infiltration & necrosis surrounded by granulation tissue
Risk factors • Opportunistic pathogen In immunocompromised host
NOCARDIA • May be cutaneous, subcutaneous or systemic lesions in humans • Pulmonary form is MC • Occurs by inhalation of bacilli • Common cause of pneumonia in immunocompromised hosts • Disseminated nocardiosis- brain abscess • Actinomycetoma: chronic granulomatous subcutaneous infection
LABORATORY DIAGNOSIS • Specimen: sputum, pus • Macroscopic examination of pus • Granules are soft • Microscopy by Gram and ZN stain(1% H2SO4) • Isolation done on routine media. • Colonies are dry to chalky, yellowish.
Histopathological examination shows multilobulated with sun ray appearance
TREATMENT • MEDICAL Rx- sulfa drugs like TMP-SMX • SURGICAL Rx- drainage of abscess