Download
1 / 1
10 likes | 194 Views
EPR Networks and Videolinks. Epilepsy Quality and Care Programme National Clinical Lead: Colin Doherty Programme Manager: Sharon Marrow sharonmorow@rcpi.ie.

E N D
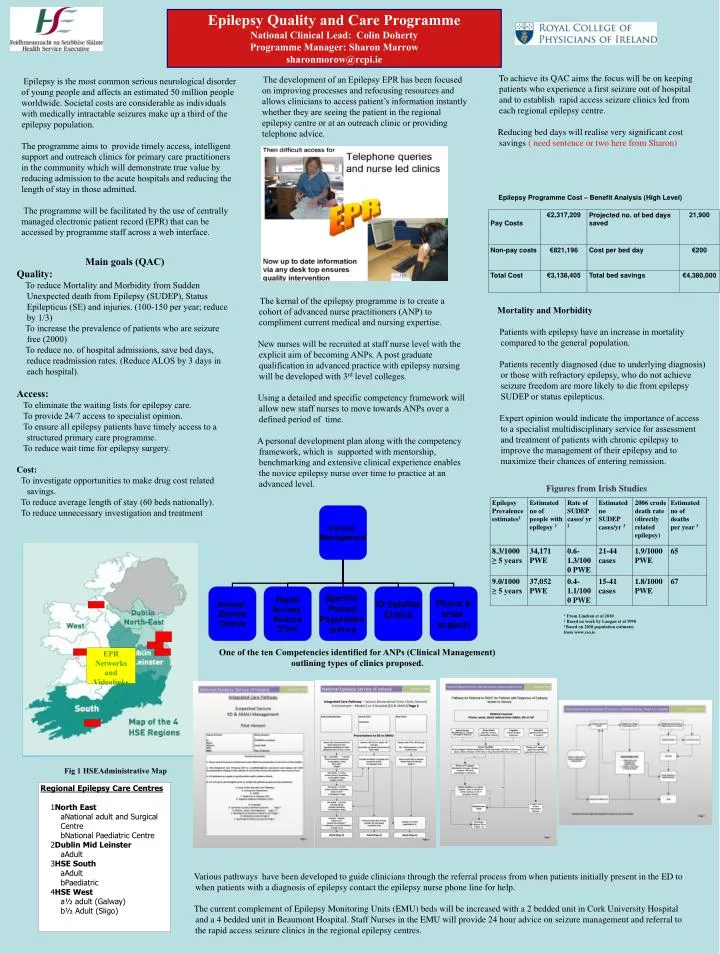
EPR Networks and Videolinks Epilepsy Quality and Care Programme National Clinical Lead: Colin Doherty Programme Manager: Sharon Marrow sharonmorow@rcpi.ie To achieve its QAC aims the focus will be on keeping patients who experience a first seizure out of hospital and to establish rapid access seizure clinics led from each regional epilepsy centre. Reducing bed days will realise very significant cost savings ( need sentence or two here from Sharon) The development of an Epilepsy EPR has been focused on improving processes and refocusing resources and allows clinicians to access patient’s information instantly whether they are seeing the patient in the regional epilepsy centre or at an outreach clinic or providing telephone advice. .Epilepsy is the most common serious neurological disorder of young people and affects an estimated 50 million people worldwide. Societal costs are considerable as individuals with medically intractable seizures make up a third of the epilepsy population. The programme aims to provide timely access, intelligent support and outreach clinics for primary care practitioners in the community which will demonstrate true value by reducing admission to the acute hospitals and reducing the length of stay in those admitted. The programme will be facilitated by the use of centrally managed electronic patient record (EPR) that can be accessed by programme staff across a web interface. Epilepsy Programme Cost – Benefit Analysis (High Level) Main goals (QAC) Quality: To reduce Mortality and Morbidity from Sudden Unexpected death from Epilepsy (SUDEP), Status Epilepticus (SE) and injuries. (100-150 per year; reduce by 1/3) To increase the prevalence of patients who are seizure free (2000) To reduce no. of hospital admissions, save bed days, reduce readmission rates. (Reduce ALOS by 3 days in each hospital). Access: To eliminate the waiting lists for epilepsy care. To provide 24/7 access to specialist opinion. To ensure all epilepsy patients have timely access to a structured primary care programme. To reduce wait time for epilepsy surgery. Cost: To investigate opportunities to make drug cost related savings. To reduce average length of stay (60 beds nationally). To reduce unnecessary investigation and treatment The kernal of the epilepsy programme is to create a cohort of advanced nurse practitioners (ANP) to compliment current medical and nursing expertise. New nurses will be recruited at staff nurse level with the explicit aim of becoming ANPs. A post graduate qualification in advanced practice with epilepsy nursing will be developed with 3rd level colleges. Using a detailed and specific competency framework will allow new staff nurses to move towards ANPs over a defined period of time. A personal development plan along with the competency framework, which is supported with mentorship, benchmarking and extensive clinical experience enables the novice epilepsy nurse over time to practice at an advanced level. . Mortality and Morbidity Patients with epilepsy have an increase in mortality compared to the general population. Patients recently diagnosed (due to underlying diagnosis) or those with refractory epilepsy, who do not achieve seizure freedom are more likely to die from epilepsy SUDEP or status epilepticus. Expert opinion would indicate the importance of access to a specialist multidisciplinary service for assessment and treatment of patients with chronic epilepsy to improve the management of their epilepsy and to maximize their chances of entering remission. Figures from Irish Studies 1 From Linehan et al 2010 2 Based on work by Langan et al 1998 3 Based on 2010 population estimates from www.cso.ie One of the ten Competencies identified for ANPs (Clinical Management) outlining types of clinics proposed. Fig 1 HSEAdministrative Map • Regional Epilepsy Care Centres • North East • National adult and Surgical Centre • National Paediatric Centre • Dublin Mid Leinster • Adult • HSE South • Adult • Paediatric • HSE West • ½ adult (Galway) • ½ Adult (Sligo) Various pathways have been developed to guide clinicians through the referral process from when patients initially present in the ED to when patients with a diagnosis of epilepsy contact the epilepsy nurse phone line for help. The current complement of Epilepsy Monitoring Units (EMU) beds will be increased with a 2 bedded unit in Cork University Hospital and a 4 bedded unit in Beaumont Hospital. Staff Nurses in the EMU will provide 24 hour advice on seizure management and referral to the rapid access seizure clinics in the regional epilepsy centres.