Download
1 / 33
340 likes | 601 Views
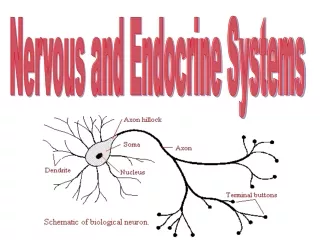
DIFFUSE HORMONAL SYSTEMS AND ENDOCRINE TUMOR SYNDROMES. Hasan AYDIN, MD ; Yeditepe University Medic al Faculty; Department of Endocrinology and Metabolism. THE ORIGIN OF NEUROENDOCRINE TUMORS. NET originates from APUD ( Amine Precursor Uptake and Decarboxylation ) cells.

E N D
DIFFUSE HORMONAL SYSTEMS AND ENDOCRINE TUMOR SYNDROMES Hasan AYDIN, MD; Yeditepe University Medical Faculty; Department of Endocrinology and Metabolism
THE ORIGIN OF NEUROENDOCRINE TUMORS • NET originates from APUD (Amine Precursor Uptake and Decarboxylation) cells. • APUD cells constitute the diffuse endocrine system of the body. • Gastrointestinal tractus • Pancreas • Lung • Central nervous system • Skin • Adrenal medulla • Thyroid
Neuroendocrine Tumors Frequency • Incidence: 1-2/100.000 • Autopsy series 8/100.000 • Carcinoid tumors are the most frequent type. (40% of all NETs)
CLASSIFICATION OF NET • Well differentiated neuroendocrine tumor • Well differentiated neuroendocrine carcinoma • Poorly differentiated neuroendocrine (small cell) carcinoma • Mixed endocrine tumors WHO International Histological Classification of Tumours, Springer Verlag 2000
Classification of NETs of GEP system • Carcinoid tumors • Foregut • Bronchial carcinoid tumors • Gastric carcinoid tumors • Midgut • Small intestinal carcinoid tumors • Apendix carcinoid tumors • Hindgut • Rectal carcinoid • Pancreatic endocrine tumors • Insulinoma • Gastrinoma • Glucagonoma • VIPoma • Somatostatinoma • PPoma
Carcinoid Tumors • Analyses of 13,715 cases of carcinoid between 1950-1999 in USA: 75% located in gastrointestinal system 25% located in bronchopulmonary system.
Carcinoid Syndrome • Carcinoid syndrome: • Vasomotor symptoms • Flushing • Tachycardia • Hypotension • Sweating • Gastrointestinal hypermotility (diarrhea) • Bronchospasm (wheezing, dispne) • Carcinoid syndrome is seen in 10% of all gastrointestinal carcinoid tumors.
Gastric Carcinoid Tumors • Constitute 4.1% of all carcinoid tumors and less than 1% of all gastric neoplasms. • Most frequently seen between age 50-60. • There are 3 distinct types: • Type 1: Associated with Type A chronic atrophic gastritis • Type 2: Associated with Zollinger-Ellison syndrome • Type 3: Sporadic gastric carcinoid tumors
Pancreatic Endocrine Tumors • Estimated incidence 1-4 / 1.000.000. • Can be a part of MEN-1 syndrome. • Clinical presentation varies according to the hormone(s) secreted.
Insulinoma • Mostly seen in the 5-6 decades. • Symptoms of hypoglycemia • Palpitation, sweating, nervousness, conscious disorders, coma etc • The tumor size usually <1.5 cm. • Usually cannot be detected with CT, MRI and angiography. • EUS is the best method for pre-op localization of the tumor. • Per-operative palpation and IOUS are the best methods to identify the tumor.
Gastrinoma • Usually presents with abdominal pain due to peptic ulcer and diarrhea due to hypersecretion. • Ulcers are seen in stamach, duodenum, esophagus and intestines. • Gastrinomas are associated with MEN-1in 25% of the cases. • Fasting gastrin level >100 pg/ml. • Basal acid secretion is >15 mEq/hour. • PPI are effective in supression of acid secretion
Somatostatinoma Frequency ( % ) Sign/Symptom Pancreatic (n=27) Intestinal (n=21) Diabetes Mellitus 95 21 Gallbladder disease 94 43 Diarrhea 92 38 Steatore 83 12 Hypochlorhydria 86 17 Weight loss 90 69
Diagnosis of Neuroendocrine Tumors • Depends on each cellular type • For correct diagnosis: • Clinical symptoms • Humoral biochemical tumor markers • Stimulant(Provacative) tests • Imaging techniques • Histopathology (CgA, sinaptofizin, NSE)
Biochemical Tumor Markers • Biochemical markers for NET: • Nonspecific marker: Plazma Chromogranin A (CgA) • Specific marker(for carcinoid): 24-hour urine 5-HIAA
Provocation Tests for GEP/NET Tumor Provacation tests Carcinoid Pentagastrin test Gastrinoma Secretin test Insulinoma Extended fasting glucose test VIPoma None Glucagonoma None Somatostatinoma None
Advantages High sensitivity. Whole body imaging. Predicts response to octreotide therapy. Disadvantages Cannot detect tumors not expressing somatostatin receptors Octreotide Scintigraphy -Somatostatin receptors including subtype 2 (sst-2) are present in 88-100% of carcinoid tumors. -Lower tumor size limit 0.5 cm. -Sensivity is around 90%.
Imagingof Neuroendocrine Tumours • Ultrasound: low sensitivity for primary ~30%; metastases ~70% • Spiral CT vs MRI: primary up to 70%; metastases 90% • Octreotide scan: primary up to 80%; 95% metastases • Endoscopic Ultrasound: ~95% pancreatic primary tumour gastric carcinoid; rectal carcinoid
Insulinoma Potassium replacement IV dextrose administration Diazoxide Gastrinoma Correction of performance status Control of bleeding Control of hyperasidity (proton pump inhibitors) VIPoma Fluid replacement Acid- base and electrolyte correction Glucagonoma Correction of the nutritional status Blood transfusion Control of hyperglycemia Somatostatinoma Correction of the nutritional status Control of hyperglycemia Symptom Control– General Measures
Systemic Treatment • Chemotherapy • Interferon alpha • Somatostatin analogues • Radioactive labelled • Somatostatin analogues • MIBG
Combination Chemotherapy • Streptozocin-5-fluorouracil • Streptozocin-Doxorubicin • Streptozocin-5-fluorouracil-Doxorubicin • Cisplatinum-Etoposide • 5-Fluorouracil-Doxorubicin-Cisplatinum • 5-fluorouracil-leucovorin-Interferon
Chemoembolisation • Indicated in unresectable liver mets • May provide symptom and clinical syndrome control • May result in tumor proliferation control • Contraindications: • Liver failure • Ascites • Renal failure • Portal vein obstruction
Biological Treatment • Somatostatin analogues • Octreotide • Lanreotide • SOM230 • Interferon • Interferon alfa-2a (Roferon-A) • Interferon alfa-2b (Intron A)
INTERFERON TREATMENT:Controversies: • No concensus on the dose and regimen to be used • No randomized trial showing improvenment of survival with interferon
SOMATOSTATIN ANALOGUES • Octreotide – Sandostatin • Lanreotid- • Somatuline-BIM 230146 • SOM230 • Octastatin- RC-160 • Somatostatin analogues are used in the treatment of carcinoid tumors and functional islet cell tumors of the pancreas
OCTREOTIDE FOR TREATMENT OF NET • Somatostatin analogues provide: • Symptomatic response : % 70 • Biochemical response : % 30-50 • Tumor control : % 3 Di Bartolomeo, Cancer, 1996.
MIBG - META-IODOBENZYLGUANIDINE Is an catecolamine analog used in localization of adrenal medulla and nonmeduller NET 123I labelled MIBG is used for diagnostic purposes Kaltas et al, J Clin Endocrinol Metab, 2001 12 pts 11/12 111In-pentetreotide positive 1/12’si 123I-MIBG (+) 123I-MIBG may be done to select patients for 131I-MIBG radionuclide therapy
TUMOR TARGETED RADIOACTIVE SOMATOSTATIN TREATMENT • Alpha-emitting radioligands • Short acting auger electrons are used 111 In-pentetreotide • Beta-emitting radioligands • High energy beta particules • 90Y-DOTA0 Tyr3-octreotide (OctreoTher) • 177Lu-DOTA0 Tyr3-octreotate • 90Y-lanreotide • Can only be used in sst2 and sst5 (+) NET de Herder et al, Curr Opin Oncol, 2002
Bortezomib(PS-341): May increase progression free survival Endostatin Thalidomide Bevacizumab: Increased progression free survival, however biochemical control was better in the interferon arm Imatinib PFS survival was significantly better in patients with concurrent octreotite SU11248 showed clinical activity in NETs Gefinitib Produced prolonged disease stabilization Temsirolismus Stabilization of diesase was observed in patients with progressive diease under various medical treatments.
Multiple Endocrine Neoplasia • MEN 1 • Pituitary adenoma • Pancreatic endocrine tumor • Parathyroid neoplasia (90%) • MEN 2a • Medullary thyroid cancer (100%) • Pheochromocytoma (50%) • Parathyroid neoplasia (10-40%) • MEN 2b • Medullary thyroid cancer (100%) • Pheochromocytoma (50%) • Neuromas (100%)
Multiple Endocrine Neoplasia Type 1 • Primary hyperparathyroidism 90% • Pituitary tumours 20-40% (90% at autopsy) • Pancreatic endocrine tumours 30-70%; (carcinoid 10%) • Chromosome identified 11q13 (LOH) • MEN-1 gene cloned 1997 • Makes protein MENIN which affects speed of cell growth/replication
Von Hippel Lindau • phaeochromocytoma, retinal/cerebellar haemangioblastoma, renal and pancreatic tumours, middle ear tumours • pancreatic NETs 15-20% - especially non-functional and PP, SST positive tumours • chromosome 3 short arm • VHL protein involved in regulation of cell replication • NETs also described in Recklinghausen disease, Tuberous Sclerosis