Download

1 / 32
360 likes | 572 Views
What do we need from clinical audit to support quality improvement?. RCP, since 2011 Safe Care team, QIPP programme, DH, 2010/11 Health Foundation Quality Improvement Fellow, Institute for Healthcare Improvement, Boston, USA 2009/10* Masters in Public Health, Harvard, 2009/11

E N D
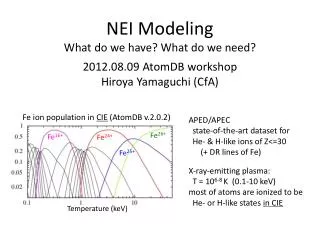
What do we need from clinical audit to support quality improvement? Kevin Stewart MPH FRCP FRCPI Clinical Director Clinical Effectiveness & Evaluation Unit Consultant Geriatrician, Winchester
RCP, since 2011 Safe Care team, QIPP programme, DH, 2010/11 Health Foundation Quality Improvement Fellow, Institute for Healthcare Improvement, Boston, USA 2009/10* Masters in Public Health, Harvard, 2009/11 Medical Director, Winchester & Eastleigh NHS Trust, 2005/09 Consultant Geriatrician, since 1990 Sources; OECD, Commonwealth Fund, Health Foundation, Kings Fund, Nuffield Trust, Institute for Healthcare Improvement *Health Foundation funded
Every healthcare system struggles with… • Increasing costs • Poor quality • Variability ..in addition, we all have some specific local issues, related to culture, politics, context etc
In the UK we face… Generic issues • Rising costs, poor quality, variability Specific UK issues • Lower baseline spending (9.6% GDP) • Higher efficiency expectation than most • …but higher recent growth than most
Top down • Regulatory & legal • Inspection, CQC, duty of candour • Compliance measures, safety alerts • Targets and directives (MRSA etc) • National campaigns • Using the payment mechanisms • QOF • Non payment for “Never events” • CQUINs, Best Practice Tariff in NHS England • Setting and modelling culture
Using the payment system? • Policymakers overestimate the power of payment systems • The UK uses it more than most • All systems have unintended consequences • There is poor alignment of incentives • There is a limit to the proportion of income which can be linked to payment • Introducing new models is more difficult and takes longer than anticipated *Payment system reform; lessons for the UK from Europe; Nuffield Trust 2012 See also Dornan et al. BMJ 8/3/14 and Daniel Kahneman, Thinking Fast & Slow
Culture and behaviour in the English National Health Service Dixon-Woods et al BMJ Q&S Sept 9, 2013 “Consistent achievement of high-quality care was challenged by unclear goals, overlapping priorities that distracted attention, and compliance-oriented bureaucratised management. The institutional and regulatory environment was populated by multiple external bodies serving different but overlapping functions”.
Bottom up • “Industrial” Quality Improvement approaches (PDSA, Lean etc) • Professional initiatives (Audit, accreditation, guidelines and protocols) • Confidential enquiries Patient-directed • Public reporting of outcomes • (?the market??)
“Industrial” approaches to QI Developed from manufacturing industry Different approaches with common features Lean, Six Sigma, PDSA, statistical process control Some high profile healthcare organisations have adapted them at scale Intermountain Health, Kaiser Permanente in US (Sheffield model for elderly care in the UK*) *Tom Downes model on Kings Fund website, Oct 2013
Common features of successful QI projects A focus on data and measurement Understanding the process and improving reliability Understanding demand, capacity, flow Partnerships with patients Adaptation for local context and culture Engaged leadership Involved and engaging staff
Common features of unsuccessful QI projects • Poor engagement of clinicians and frontline staff • Inadequate strategy for spread and sustainability • Poor alignment with policy and strategy drivers • Working in isolation • No adjustment for local context…… See SPI evaluation, BMJ Feb 3, 2011
Do the public make choices on the basis of reported outcomes? “In every other walk of life choice and competition and diversity drive up quality standards” ???
Public reporting of health outcomes *Marshall & McLoughlin BMJ 11 Dec 2010 * Boyce, Dixon, Fasolo ,Reutskaja King’s Fund 2010
Public reporting of health outcomes • Patients tend to choose based on; • Personal experience • Recommendations of friends and family • Convenience/locality • ..but public reporting may lead to improved quality indicators, through; • Data “cleaning”, case selection etc • Competition between providers and cross-learning leading to genuine improvements
Improving quality The “best” approach? • Probably a mixture of all • alignment of external rewards, incentives and penalties • with intrinsic (professional) motivation • Making the right thing easier • Removing barriers to high quality • Top down for compliance • Bottom up for commitment
National clinical audits…. • Seem to work best when they seek to influence at different levels • National policy • Regulatory/commissioning • Local QI • Adapt depending on their degree of maturity
Early stage clinical audits… • Get the topic on the local and national policy agenda • Provide data • The big picture is more important than local performance • Energize clinicians • Interest clinical leaders • Engage patient and voluntary groups
As audit matures… • More focus on methodology and data quality • Data expected to be used more widely by; • Organizational leaders, policymakers • Regulators and commissioners • Press and the public • Move from organizational to process and outcome measures • Concerns about burden of data collection/alignment with other work/other measures
Where can we develop further? • Reducing the burden of data collection • Aligning with existing (imperfect) data sources • Aligning across audits • Thinking beyond the “mega-database” model • Patient reported measures • Reader-friendly presentation of outputs
Summary This stuff is difficult beware “simple” solutions to complex problems “Top down” gets compliance, but for commitment we need to grow “bottom up” Clinical audit needs to mature and develop to accommodate changing demands
Acknowledgements • The Health Foundation, London • Jim Conway and others at Institute for Healthcare Improvement, Cambridge, MA • Colleagues at RCP London • Clinical colleagues in Winchester for their patience, flexibility and tolerance! Kevin.stewart@rcplondon.ac.uk
Useful references Institute for Healthcare Improvement www.ihi.org The Health Foundation www. health.org.uk The Commonwealth Fund For in depth view of US system and international comparisons www.commonwealthfund.org Wachter’s World website and blog Nuffield Trust and King’s Fund websites Rcplondon.ac.uk (national audits and quality improvement programmes in stroke, falls, continence, IBD etc) Kevin.stewart@rcplondon.ac.uk