Download
1 / 27
490 likes | 1.33k Views
Thyroid Drugs. Kaukab Azim, MBBS, PhD. Learning Outcomes. By the end of the course the students should be able to discuss in detail Physiology, synthesis and feed back control of thyroid hormone synthesis Thyroid disorders: Hypothyroidism Cretinism, Myxedema coma Hyperthyroidism

E N D
Thyroid Drugs Kaukab Azim, MBBS, PhD
Learning Outcomes By the end of the course the students should be able to discuss in detail • Physiology, synthesis and feed back control of thyroid hormone synthesis • Thyroid disorders: • Hypothyroidism • Cretinism, Myxedema coma • Hyperthyroidism • Thyroid storm • Drugs for the treatment of hypothyroidism and hyperthyroidism
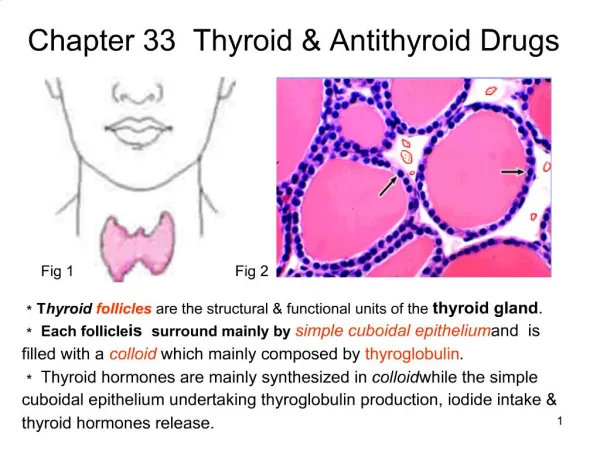
Thyroid Hormones • Thyroid hormones: • Thyroxine T4 (90%) • Triiodothyronine T3 • Thyroid gland also secretes Calcitonin – serum calcium lowering hormone
Thyroid Hormones - Facts • Thyroid hormones are required for the growth and development of all tissues. • Thyroid hormone is critical for nervous, reproductive and skeletal growth. • Thyroid deprivation in early life results in irreversible mental retardation. • Thyroid hormones also augment sympathetic system function primarily by increasing the number of adrenergic receptors.
TSH secretion by anterior pituitary is stimulated by hypothalamic TRH Feedback inhibition of TSH and TRH occurs with high levels of circulating thyroid hormones (T3 & T4) Dopamine, Glucocorticoids and somatostatin can suppress TSH secretion Hypothalamus-pituitary-thyroid axis (High dose)
Thyroid hormone synthesis • Uptake of iodide by thyroid gland • Oxidation of iodide • Organification • Iodination of tyrosine residues on thyroglobulin • MITs and DITs • Coupling – formation of T4 and T3 • Proteolysis of thyroglubulin and secretion of thyroid hormones • Conversion of T4 to T3 in peripheral tissues
Thyroid hormone synthesis T4 TBP T3 & Free T4 & T3 (Iodide Organification) 4. Coupling
Metabolism of thyroid hormones Outer ring Inner ring (T4) 5’-deiodinase (4X potent than T4)
Metabolism of Thyroid hormones Drugs that inhibit deiodination: • Beta blockers • High dose propylthiouracil • Corticosteroids • They inhibit the 5’-deiodinase activity necessary for conversion of T4 to T3 resulting in low T3 and high reverse T3 (rT3)
T4 and T3 must dissociate from thyroxine binding globulin (TBG) in plasma before entering into the cells. In the cells, T4 is deiodinated to T3 that enters nucleus and attaches to specific receptors which promotes mRNA and protein synthesis. Thyroid hormones Mechanism of action
Hypothyroidism Clinical manifestations: • Lethargy • Wt. gain • Bradycardia • Constipation • Cold intolerance • Menstrual irregularities • Cretinism (congenital hypothyroidism) • Myxedema coma: most extreme manifestations of untreated hypothyroidism
Levothyroxine (T4) It is the treatment of choice for replacement therapy in hypothyroid patients It has a long half life ~7 days; once a day dose. Triiodothyronine(T3) Short half life (1 day) Drugs for Hypothyroidism
Drugs for Hypothyroidism • T4 and T3 given orally. • T4 is better for long term replacement therapy • I.V. administration in myxedema coma • During pregnancy, hypothyroid woman require higher doses
Hyperthyroidism • Clinical manifestation • Weight loss and with increase in appetite. • Nervousness and irritability. • Palpitations. • Heat intolerance and increased sweating. • Tremors. • Thyroid enlargement • Menstrual irregularities
Hyperthyroidism Treatment options: • Surgical • Antithyroid drugs: • By inhibiting uptake of iodine • By inhibiting synthesis • By inhibiting release of hormones from thyroid • Medical destruction of thyroid tissue • Radioiodine (I131)
(-) Anion Inhibitors T4T3 5’-deiodinase (-) Propylthiouracil, Ipodate, beta blockers, cortocosteroids
1. Thioamides Propylthiouracil, Methimazole • Inhibit hormone synthesis • Acts by inhibiting thyroid peroxidase to block iodine organification and coupling reactions • These are the major drugs for treatment of mild thyrotoxicosis and in preparation of patients for subtotal thyroidectomy
Thioamides • Slow onset of action (~ 4 weeks) • Propylthiouracil is relatively safe and preferred in pregnancy • Methimazole is more potent and longer acting than Propylthiouracil • Propylthiouracil also inhibits peripheral deiodination of T4 and T3
Thioamides: Adverse drug reactions • Common:Maculopapular Rash, Arthralgia, vasculitis • Serious side effect: Agranulocytosis
2. Iodides:Potassium iodide, Lugol’s solution • Mechanism of action • Inhibit hormone release • Inhibit organification • Decrease size and vascularity of the hyperplastic gland. • Effect is reversible and transient – not for long term as thyroid gland ‘escapes’from its effect after 14 days • Contraindicated in pregnancy: fetal goiter
3. Iodinated contrast media Ipodate and Iopanoic acid • They inhibit the peripheral conversion of T4 into T3 in the liver, kidney and brain • Inhibition of hormone release is an additional mechanism • Adjunctive therapy in the treatment of thyroid storm
4. Anion Inhibitors Perchlorate (ClO4-), Pertechnetate (Tco4-), Thiocyanate (SCN-) • competitively block the uptake of iodide • Adverse effect: Aplastic anemia
5. Radioactive Iodine • 131I is the only isotope used in treatment of thyrotoxicosis while others are used in diagnosis. • Emission of beta particles – destroys the thyroid gland. • Patients can become hypothyroid – managed with thyroxine (T4) • Contraindications: • Pregnancy & lactation • Age <25 yrs
Thyroid storm • Clinical manifestation • High fever often above 40°C • Fast and often irregular heart beat • Vomiting, diarrhea and agitation. • Heart failure and myocardial infarction may occur. • Death may occur despite treatment. • Causes • Patients with known hyperthyroidism whose treatment has been stopped or become ineffective, • Untreated mild hyperthyroidism who have developed an intercurrent illness (such as an infection).
Thyroid storm Treatment • Propranolol /Esmolol / Diltiazem • Iodide/ipodate – ipodate also block the T4 to T3 conversion • Propylthiouracil • Hydrocortisone – blocks the T4 to T3 conversion