Download
1 / 11
110 likes | 308 Views
Saka Kazeem MD, CMD Arlene Latimer MS, RN Dorette Smith, RN Annett Ford, RD, RN Igor Kiprovski, Assoc. Administrator. Skilled Nursing Facility : The New Med Surg. An Integrated Approach in Reducing Hospitalizations Through Value Based Healthcare. Speaker Disclosures.

E N D
Saka Kazeem MD, CMD Arlene Latimer MS, RN Dorette Smith, RN Annett Ford, RD, RN Igor Kiprovski, Assoc. Administrator Skilled Nursing Facility: The New Med Surg. An Integrated Approach in Reducing Hospitalizations Through Value Based Healthcare.
Speaker Disclosures None of the speakers for the Center of Nursing & Rehabilitation have any relevant financial relationship with any vendors of products or programs mentioned in this presentation.
Learning Objectives By the end of the session, participants will be able to: • Assess current systems and identify top 5 re-hospitalization drivers in long and short term/sub-acute settings. • Identify and develop collaborative interdisciplinary strategies and plans for hospitalization reduction. • Implement innovative systems and protocols to capture key clinical metrics and improve clinical outcomes. • Foster an integrated partnership among key business stakeholders to identify best practices and create a formalized value based hospitalization reduction process.
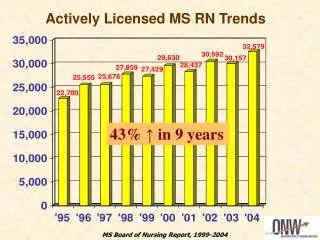
Background and Benchmark Data The Center for Nursing & Rehabilitation, located in the Prospect Heights section of Brooklyn, New York, is a 320 bed not-for-profit facility and a member of the Center Light Health System. The Facility has a dedicated 40 bed Sub-acute Care Unit, with 40 beds allocated for medically complex residents. The remaining 240 beds serve the needs of resident with a variety of physical co-morbidities and cognitive challenges. The facility reviewed the less than 30 day re-hospitalization data from January 1, 2010 through December 31, 2010 for patients admitted to the short term/sub-acute unit. The data identified that the facility had an annual average re-hospitalization rate of 32%, significantly higher than the New York State (21.89%), and Kings County average (29.58%). The facility had a 97.21% average annual occupancy rate with residents’ acuity levels at an average case mix index score of 1.01.
Cycle One (January-June 2011) Concerns: • Inadequate tools in capturing dynamic changes in short term/sub-acute residents condition. • Ineffective communication between physicians and licensed nurse • Need to improve staff clinical competency Action Steps: • Review of current assessment tools, policy and procedures and competency of clinical staff. • Facility embarked on a six (6) week intensive training for all licensed nursing staff working on the sub-acute and medically complex unit. • Implementation of INTERACTNY tools: SBAR, Stop and Watch. • Weekly classes held by the Medical Director focused on education of the nursing staff on topics self identified as requiring further development. • Develop algorithms and protocols for the incidence of severe hyper/hypo glycemia. • Develop and implement protocol for IV Lasix Therapy. Outcome: 22% reduction in the less than 30 day re-hospitalization rate for patients on the short term/sub-acute unit as compared to our 2010 benchmark data.
Cycle Two (July-December 2011) Concerns: • Medication reconciliation process did not adequately capture the true medication profile of our patients. • Lack of medication reconciliation process prior to discharge, resulting in potential poly pharmacy. • Lack of reconciliation for medications taken prior to hospital and skilled nursing facility admission. • Facility did not have an Anemia and Low Hemoglobin hospitalization risk assessment. Action Steps: • Medication reconciliation process was revised to expand our focus on not only the hospital medication list and what is ordered in the nursing home, but to include medications that the patient was taking prior to admission to the hospital. • Patients diagnosed with anemia or low hemoglobin were identified as high risk for re-hospitalization due to the need for transfusion. The facility developed a relationship with an outpatient, local hospital sponsored, infusion center and developed a transfusion policy and protocol. Outcome: • Improved and adequate medication reconciliation process was developed to appropriately capture the true medication profile of our patients. • Transfer of patients to the infusion center for treatment and have them return to the nursing home rather than being hospitalized.
Cycle Three (January-June 2012) Concerns: • Long Stay Resident Hospitalizations were high. 944 hospitalizations per 1,000 resident days. • Culture of Hospitalize rather than treat in place – clinical staff. • Hospitalization Risk assessment tool for short term/sub-acute patients did not exist. • System of hospitalization notification and review did not exist. • Advanced Directives • Communication with Partnering Hospitals Action Steps: • Review of current risk assessment tools, policy and procedures and developed new risk assessment tool to identify short stay patients at high risk for re-hospitalization. A modification of the Karnofsky scale dubbed the Baccash Acuity Scale was developed. • Focused “Culture Change” education sessions with the Nursing and Medical staff to anchor the treat in place mantra. • A patient transfer policy was developed to establish communication protocols which include notification of the Medical Director whenever a hospitalization is initiated. • Monthly video conference meeting was established with our partnering hospital. The Medical Director, Director of Nursing and pertinent nursing staff from the nursing home digitally meet with the Assistant Chief Medical Officer and Chief of case management from the hospital to discuss Medical Issues that could have been addressed in the hospital and Medical issues that could have been addressed in the nursing home. • Hospital partnered with the nursing to focus on advanced directives. Outcome: 28% reduction in the less than 30 day re-hospitalization rate for patients on the short term/sub-acute unit as compared to our 2010 benchmark data.
Cycle Four (July-December 2012) Concerns: • Sustainability of implemented action steps in cycles 1-3. • Patients with dislodged Gastrostomy Tubes. Action Steps: • Stop and Watch program expanded to both the clinical and non clinical team. • Monthly (Short-term) and weekly (long term) video conferencing sessions are held with our primary business partners. • Advanced Directive initiative had been instituted to address hospitalizations caused by the transfer of patients to the hospital for end-of-life care which could have been provided at the skilled nursing facility. • Treat in place initiative evolved to include evening Physician rounds, Gastrostomy Tube insertions and an on site electrocardiographic evaluation of patients exhibiting cardiac related symptoms, such as chest pain. • Develop GT Tube policy and protocol • Diabetic management algorithm was reviewed and further revised to include not only severe cases of hyper/hypo glycemiabut rather all episodes. Outcome: 28% reduction in the less than 30 day re-hospitalization rate for patients on the short term/sub-acute unit as compared to our 2010 benchmark data. External Patient satisfaction survey rating 95% with a recommended rating of 97%.
Conclusion Generalizability The approaches outlined in this Initiative can easily be implemented by any other Long Term care Facility. The steps include: • Review of current screening/assessment tools • Revision/implementation of communication tools • Review and revision of facility policy and procedure to align with any identified revisions • In-Service staff in fundamental hospitalization reduction concepts and revised approaches • Provide focused education on medical management for complex cases • Establish collaborative partnerships with primary business partners • Include interdisciplinary team in decision making process • Review the facility’s policies and procedures addressing advanced directives to ensure best practice and compliance with regulations • Share the results of your efforts • Celebrate your success Impact of the Long Term Care Facility • Reduction in the hospitalization rate • Increase in staffs’ education and competency • Improve communication and trust between the interdisciplinary team. • Improved communication and trust with our business partners. • Increase in facility’s occupancy rate • Increase in acuity level
Accomplishments Long Stay Hospitalization Outcomes Facility Short Stay Annual Outcomes *2013 data reflects Quarter 1 and Quarter 2 results Less than 30 Day Re-Hospitalization Rate Comparison Facility Commitment The Center for Nursing and Rehabilitation adapts a multidisciplinary approach to reducing re-hospitalization, by implementing a comprehensive medical approach with the objective to manage and treat in place. The team spear headed by the medical directors was committed to improving the competency of the Medical and nursing staff.