Download
1 / 49
490 likes | 713 Views
CERVICAL SPECIFIC PROTOCOL FOR 100 MENIERE’S PATIENTS. THE 25 th ANNIVERSARY OF THE PROSPER MENIERE SOCIETY The 12 th International Symposium and Workshops on Inner Ear Medicine and Surgery. Prosper Meniere 1861. Director of the Paris Institute for Deaf-Mutes

E N D
CERVICAL SPECIFIC PROTOCOL FOR 100 MENIERE’S PATIENTS THE 25th ANNIVERSARY OF THE PROSPER MENIERE SOCIETY The 12th International Symposium and Workshops on Inner Ear Medicine and Surgery
Prosper Meniere 1861 • Director of the Paris Institute for Deaf-Mutes • First described the condition that was later named for him
Andrew Taylor Still, MD, Founder of Osteopathy • Watched three of his children die of spinal meningitis in the 1870’s, after being treated by having their skin burned with hot irons and having leeches applied to their open wounds • Bloodletting was the most common medical treatment at that time
Wilhelm Conrad Roentgen • Took the first x-ray in October 1895 of his wife Frau Bertha’s hand • Awarded the first Nobel Prize in Physics 1901 • Later, his wife’s hand was amputated and soon after she died of cancer caused by his experiments
Harvey Lillard, September 18, 1895 • Black male janitor presented with almost total deafness • Case history: he was working in a stooped, cramped position when he felt something pop and heard a crack in his neck, immediately losing his hearing
D.D. Palmer, Magnetic Healer • Discovered a bump on the back of Mr. Lillard’s neck at level of C2 (Axis) • Performed the first chiropractic adjustment • Within ten minutes Mr. Lillard’s hearing was fully restored
BJ Palmer, DC • Son of DD Palmer • Took over Palmer Chiropractic College from his father • Started researching upper cervical specific chiropractic in 1931
William G Blair, DC • Started researching the atlanto-occipital joints in 1951 • Started teaching his technique in 1961 • The Blair technique is the only non-orthogonal upper cervical specific technique today
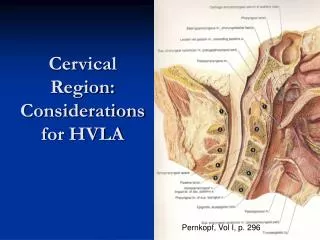
2 Superior Articulations of C1 (Atlas) • “Before you can know the correct vertebral positions, you must first know all the existing asymmetries and malformations,” William Blair.
“Subluxated articular misalignments are analyzed as they displace the neural rings, thereby occluding the neural canal and compromising the cord space,” Blair. Atlas Subluxation
My Own Experience • Dr Perry Rush, instructor at Sherman College of Straight Chiropractic, introduced me to the Blair Technique in 1995, and gave me my first upper cervical specific adjustment.
4 Blair Atlas Subluxation Listings • Anterior and Superior on the Right (ASR) • Anterior and Superior on the Left (ASL) • Posterior and Inferior on the Right (PIR) • Posterior and Inferior on the Left (PIL)
Blair X-Ray Analysis of Atlas • If the atlas “tracts” up or down on the left condyle, you will be able to see the misalignment being created and demonstrated on the right condyle.
Over lap (ASR) and the under lap (PIL) of C1 in relation to Occiput.
Next we have atlas beneath the occiput. Atlas tracts along the left condyle and will show the creation of an anterior superior right (ASR) subluxation first. It then follows through and shows…
Listings Determined by X-Ray • View lateral edges of the two articulations between Occiput and Atlas on Nasium and AP Open Mouth or Oblique Protracto Views • Overlapped Atlas determines Anterior and Superior listing on side of that articulation • Underlapped Atlas determines Posterior and Inferior Listing on opposite side of subluxated articulation
Lateral Cervical of Meniere’s Patient • Note lack of normal cervical curve with kink • Note posterior atlas • The only cause of these two findings on an x-ray is whiplash
Dr. Karel Lewit, Czechoslovakian neurologist Typed 120 Cases in 1961 • Type I (a)- Meniere’s Disease with no neck pain • Type I (b)- Meniere’s Disease involving neck symptoms • Type II- Cervical Vertigo (dizziness after head movements) • Type III- Mixed Cases of Type I & Type II
Lewit’s Proposed Causes of Dizziness • Inner ear disorders • Brain diseases • Blood supply interference to the inner ear • Direct nerve interference with balancing reflexes • Combination of the above causes
“Chiropractors refrain from assuming that the site of a symptom is the site of it’s cause. When an injury occurs in one area, the normal balance is disrupted, the body makes compensations and structural patterns are altered. Due to the laws of gravity, a new state of dynamic equilibrium is created.”
Other possible Morphologies of Atlas Subluxation causing Meniere’s • Irritates the nucleus of CN VIII, the Vestibulocochlear • Irritates the nerve root of CN VIII • Diminished blood flow from the vertebral artery • Increased CSF pressure via the cochlear aqueduct • Pressure on auditory tube • Ears at different heights/angles due to kink in the neck
My First Meniere’s Patient 1998 • 85 y.o. white female • Case history: whiplash in 1940’s, R sided Meniere’s since 1954, colostomy and mastectomy • Presented with vertigo, tinnitus, cervicalgia, LROM L arm, blindness L eye, numbness L thumb, R shoulder P!
The Merck Manual • Meniere’s disease is associated with endolymphatic hydrops • The cause is unknown • Treatment is empirical • Question? What causes the edema that causes the dilation of the membranous labyrinth?
Burcon Chiropractic Research • 2000- Upper Cervical Protocol for Three Meniere’s Patients, Journal of Vertebral Subluxation Research • Burcon Chiropractic 4362 Cascade Road, SE Grand Rapids, MI 49546 (616) 575-9990 drmburcon@aol.com www.BurconChiropractic.com
Upper Cervical Protocol for Ten Meniere’s Patients • Presented at the 9th Annual Vertebral Subluxation Research Conference, Sherman College of Straight Chiropractic in 2001
Dynamic Chiropractor 2003 • Parkinson’s Disease, Meniere’s Syndrome, Trigeminal Neuralgia and Bell’s Palsy: One Cause, One Correction
Upper Cervical Protocol forTen Meniere’s Patients • Same paper published in Upper Cervical Subluxation Complex, A Review of the Chiropractic and Medical Literature, by Kirk Ericksen. Lippincott, Williams & Wilkens, 2004
Upper Cervical Protocol for 30 Meniere’s Patients • 2005, Los Angeles, CA • Poster presentation • Exhibitor
WZZM Channel 13 • ABC affiliate in Grand Rapids, MI • Burcon Chiropractic’s Meniere’s research featured on the 6 and 11 O’clock News in 2005 • Resulted in 60 new Meniere’s patients
Protocol for 100 Meniere’s Patients • Extensive case history that includes at least two episodes of vertigo lasting at least 20 minutes each • Sensorineural hearing loss confirmed by audiometry • Tinnitus and/or • Perception of aural fullness • Patient must provide letter from ENT specialist confirming diagnoses with copy of test results
Demographics • 54 Females • 46 Males • Youngest: 9 y.o. • Oldest: 93 y.o. • Mean age: 53 y.o.
Cervical Syndromes Derifield/Thompson Cervical Syndrome Test- Hold patient’s shoes with thumbs under the heel, while applying very mild cephalic pressure. Lift the legs one inch off from the table, keeping the shoes one inch apart. Compare the welts to estimate the leg length differential. Notate differential of short leg to closest 1/8 inch. Instruct patient to slowly turn their head to the right, then to the left. If the legs change length only while turning to the right, notate the amount of change as a right cervical syndrome (RCS). If the legs change length only while turning to the left, notate the amount of change as a left cervical syndrome (LCS). If the leg length changes while turning the head in both directions, notate the total amount of change as a bilateral cervical syndrome (BLCS). If there is no change in leg length when the head is turned, there is no cervical syndrome. Perform following tests to determine which upper cervical vertebrae is subluxated.
Orthoneuro Examination • Modified “Modified” Prill Cervical Leg Check Protocol • Interactive presentation at the 11th Annual Vertebral Subluxation Research Conference • Determines which cervical vertebra to adjust • Intraexaminer repeatability tested very good • Interexaminer repeatability tested excellent
Modified Blair X-Ray Protocol • All 100 consecutive Meniere’s patients tested positive for upper cervical subluxations • 3 Cervical x-rays taken and analyzed: Lateral, A-P Open Mouth and Nasium • All 100 film studies showed evidence of upper cervical subluxation and whiplash, although cervical trauma was denied by over 50% of patients.
Level of Major Upper Cervical Subluxation • C1 (Atlas) in 96 out of 100 consecutive cases • C2 (Axis) in 4 out of 100 consecutive cases
Observation • When major symptom is vertigo with nausea, atlas is the major subluxation • When major symptom is tinnitus with ear fullness, axis is the major subluxation
Atlas Listings for 96 Meniere’s Patients • 0- Anterior and Superior on opposite side of bad ear • 1- Anterior and Superior on side of bad ear • 2- Posterior and Inferior on side of bad ear • 9- Posterior and Inferior bilaterally • 84- Posterior and Inferior on opposite side of bad ear
Most Significant Finding • The primary cause of unilateral Meniere’s disease is an atlas subluxation with a listing of posterior and inferior on the opposite side of the involved ear • This means that the atlanto-occipital articulation is subluxated on the side of the involved ear
Negative Side Effects • The only negative side effect noted was an increase in the frequency and magnitude of headaches in 3 patients, increasing in average from 2.3 to 5.7 • Headaches improved with 30 patients, decreasing in average from 5 to 2 • Headaches remained unchanged in 67, with the average staying at 3
Improvement at 3 Months – 6 Years (80 out of 100 Patients Responded)
“Comments:” • “I have felt safe enough to drive again.” • “Weaned off my meds with no Meniere’s symptoms!” • “I do not fall down anymore.” • “I do not snore anymore.” • “My wife says that I am easier to get along with.”
Suggestion • Next time a patient presents with Meniere’s symptoms • And brain tumors and MS are ruled out by MRI • Refer patient to an upper cervical specific chiropractor • Before resorting to surgery