Download
1 / 22
220 likes | 324 Views
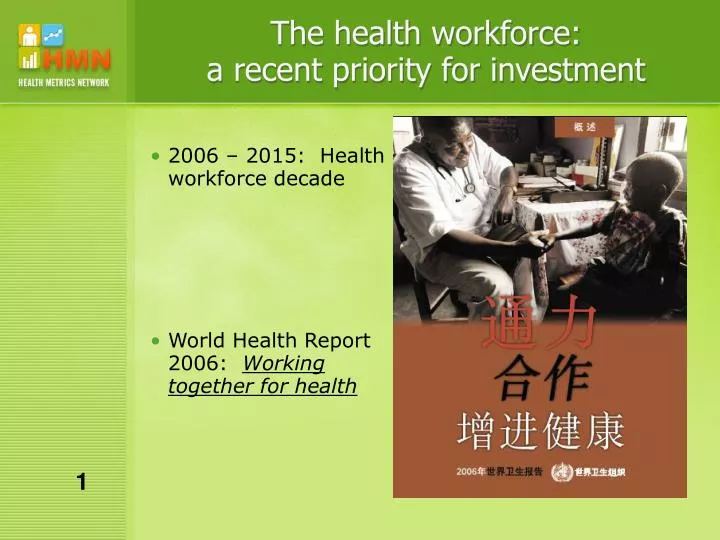
The health workforce: a recent priority for investment. 2006 – 2015: Health workforce decade World Health Report 2006: Working together for health. 1. Demand for information – What do we want to know?.

E N D
The health workforce: a recent priority for investment • 2006 – 2015: Health workforce decade • World Health Report 2006: Working together for health 1
Demand for information –What do we want to know? • Active workforce -- stocks of various types of health professionals in the public or private sectors (disaggregated by age, sex and geographic location) • Entry -- annual numbers graduating from training institutions • Exit – annual numbers departing from service due to movement to private sector, emigration, change of occupation, retirement or death 2
Demand for information –What do we want to know? • Performance -- the outputs of health workers (e.g. outpatient attendance per capita; hospitalizations per capita) • Costs -- expenditures on remuneration (including benefits) as well as on pre-service training 3
Key health workforce metrics for a health system dashboard Health worker densities • by type of health worker • by sector South African health worker densities per 100,000 Sources: HST, HSRC, NDoH, HPCSA, SANC, StatsSA 4
Key health workforce metrics if there is room on the dashboard Health worker densities • by type of health worker • by sector • by geographic location for the public sector South African health worker densities per 100,000 Sources: HST, HSRC, NDoH, HPCSA, SANC, StatsSA 5
Supply – What data sources exist? Sources of data for monitoring the health workforce (see handout) : • National population census • Labour force survey • Health facility census • Professional registration database • Civil service payroll database • Staffing reports from each health facility 6
Population census • Strengths • ·counts all workers: • - private and public • - health professionals workers working in non-health sectors • - management and support staff working in the health industry • · geographical disaggregation to lowest level • · rigorous collection and management of data • Limitations • · once each ten years • · occupational data often not coded with sufficient precision • · census authorities may be reluctant to release the micro-data • · provide little information on entry into and exit from the workforce 7
Labour force survey • Strengths • ·Counts all occupations (including management & support staff) • · Counts both public and private • · Counts unemployed and part-time workers • · Can provide information salaries & wages • · Rigorous data collection and data management. • Limitations • · Often only once each 5 years; • · Small sample size [ • Very wide confidence intervals for countries with few health workers • Geographic disaggregation often not advisable • · Occupation is often not coded with sufficient precision • · Cross-sectional: can't track entry and exit 8
Health facility census • Strengths • · counts all health facility staff including management & support staff • · allows geographical disaggregation • · can be used to track in-service training/skills and productivity • · (often) rigorous data collection and data management. • · relatively less costly • Limitations • · no data on entry and exit • · double counts dually employed workers • · may omit some private facilities, community workers, unemployed • · (historically) conducted ad hoc and infrequently • · usually don't provide data on remuneration 9
Professional registration database • Strengths • ·Counts registered health professionals (private as well as public) • · Using a unique identifier the database could track entry and exit • Limitations • · Requires developing the capacity of regulatory authorities • · Accurate updating depends upon incentives and/or enforcement • · Difficult to track non-professional health workers and support staff 10
Multiple data sources [ validation and interpolation Data on nurses in South Africa Source: HSRC, SANC, StatsSA, NDoH 11
The gap betweenSupply & Demand The Global Atlas of the Health Workforce (http://www.who.int/globalatlas/default.asp ) is now more extensively populated: • Data on more types of health workers – 2004 -- 5 occupations (physician, nurse, midwife, pharmacist, dentist) 2006 – 13 or more occupations (also clinical officer/medical assistant, radiographer, lab scientist, lab technician, dental technician, pharmaceutical technician, community health worker or TBA, health management and support workers) • Recent data for more countries – 2004 -- 48% of sub-Saharan African countries 2006 -- 96% 12
More data …but some data are now less comparable Number of physicians reported to the Global Atlas for select countries of sub-Saharan Africa 13
More data …but some data are now less comparable Number of physicians reported to the Global Atlas for Ghana Cumulative number of physicians ever trained in Ghana? Physicians registered with Ghana Medical council? MoH payroll 14
Significant inconsistencies between data sources are common Stocks of health workers in Malawi in 2004 – 2005 according to various data sources 15
Priorities for consensus on methods • Metadata must be improved: detailed information on • Source of data • Known limitations – e.g. double counting • Classification – Is private sector included?; Are health professionals working for other Ministries included? • Classification of health occupations needs further development • Revision of the ILO's ISCO • Harmonization of MoH systems of classification • Standards for disaggregation by other key variables • Sub-national location 16
Standards for disaggregation -- to compare geographic inequalities For many countries, health workforce statistics are already disaggregated by province: Physicians per 100,000 population 17
Priorities for investment in data sources • Capacity Improving health workforce statistics will require investments to build sustainable capacity of • Ministries of Health • regulatory bodies/professional councils • training institutions 18
Priorities for investment in data sources • Computerization and linkage of administrative data (on enrolment, graduation, registration/licensing, hiring, pay, deployment, transfer, promotion) Linkage possible if each worker has a unique identifier Can strengthen management as well as strategic M&E Success depends upon incentives for accurate and timely collection and reporting 19
Priorities for investment in data sources • Population census Can generate statistics on the private sector and health professionals working in non-health industries Data can be dissaggregated to the lowest level Requires census authorities to code occupational data with greater precision and grant access to the census micro-data. 20
Priorities for investment in data sources • Health facility census Can generate data on not only the human resources but their skills, productivity (volume of services provided), absenteeism, availability of other inputs (drugs, supplies, infrastructure) and quality of services. Enumeration of private facilities is a challenge Funding and political commitment needed to repeat these surveys each 2 to 3 years 21
Priorities for investment in data sources Distribution of nurses working in the public sector by district, Rwanda, SAM, 2004 22