Download

1 / 59
590 likes | 682 Views
بسم الله الرحمن الرحيم. Sepehrmanesh.z,MD. Sepehrmanesh.z,MD. نقش مداخلات خانوادگی در بازتواني روانی اجتماعي. عقاید فرهنگی درباره خانواده های افراد با ناتوانی روانی در طی 30 سال گذشته به طور واضحی تغییرکرده است.

E N D
بسم الله الرحمن الرحيم Sepehrmanesh.z,MD
Sepehrmanesh.z,MD نقش مداخلات خانوادگی در بازتواني روانی اجتماعي
عقاید فرهنگی درباره خانواده های افراد با ناتوانی روانی در طی 30 سال گذشته به طور واضحی تغییرکرده است. در حال حاضر خانوادها بیشتر به عنوان اعضاء واحد تیم باز توانی برای عضو مبتلا به ناتوانی روانی محسوب می شوند
رفاه اعضاء خانواده به طور فزاینده ای به عنوان اساس فرایند بهبودی وابستگان دارای ناتوانی روانی در نظر گرفته می شود.
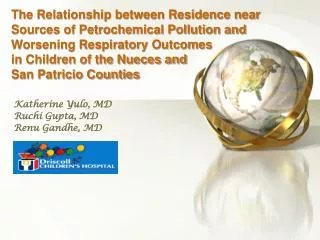
Interaction of patient symptoms and family process:A simple causal model + Family Symptoms +
Family dysfunction is now seen as a possible consequence , rather than a cause, of the illness (Lefley,1996)
در حال حاضر تأثیر آموزش خانواده در کاهش فشارهای ناشی از وجود بیمار روانی مزمن در خانواده و رفع انگ بیماری از وی در جامعه بصورت قابل ملاحظه ای مشاهده شده است.
خانواده یک مجموعه حمایتی طبیعی بوده و منبعی پربار برای توانبخشی بیمار روانی مزمن بشمار می آید. محیط خانه و خانواده موقعیت طبیعی برای آموزش توانمندی و بهبودی بیمار محسوب می شود.
مشارکت خانواده در توانبخشی بیماران روانی مزمن باعث بهبود فرایند توانبخشی - درمان و ارتقای کیفی آن می گردد و منجر به توانمندی بیمار روانی مزمن می شود.در این صورت خانواده تشویق میشود به صورت فعال در فرایند توانبخشی و درمان شرکت کند
خانواده هایی که نیازهایشان از طریق مداخلات خانوادگی مورد نظر قرار گرفته شده ازکیفیت زندگی بهتری برای خود ووا بسته مبتلا به ناتوانی روانی برخوردار می شوند
The recent recommendations specified that family interventionsshould have the key elementsof being at least 9 months in duration and including “illness education, crisis intervention , emotional support, and training in how to cope with illness symptoms and related problem.
Evidence indicates that interventions lasting less than 6 months are not as effectivein reducing relapse (Lehmanet al,.2004).
Understand unique issues of family members , including parents , spouses , siblings , offspring , and caring others . Identify impact of mental illness on family relationships and dynamics that may put members at psychological and physical risk.
شناخت خانواده از ماهیت و خصوصیات بیماری روانی مزمن و تأثیر بیماری بر فرد بیمار و خانواده قدم اولاست و در قدم بعددریافت نقطه نظرات خانواده، بررسی نیازهای خانواده و بیمار و یادگیری مهارت های فردی توسط خانواده و بیمار نقش مهمی را ایفا می کند. .
Family interventions Hatfield (1994a) has categorized these interventions as clinical and non clinical .
Clinical interventionswere developed by mental health professionals ,and nonclinical ones were mostly developed by family members. Nonclinical domain includes family support and advocacy groups, family education, family consultation, planned lifetime assistance …
Clinical interventions Psychoeducational interventions Originally , these interventions were created by mental health professionalsin response to the EE research, with the intention of enhancing the family members ability to cope with their relatives illness and thereby lowering their expressed emotion behavior .
Non clinical interventionfamily education The goals are to reduce family stress and burden, Increase family coping skills, improve family quality of life. Emphasize the competencies of families, rather than their deficits. (SOLOMON) These interventions are notbased on presumption of family pathology. Generally, are brief
Family education -Duration- a few hour-12w -Family experiences -Freestanding, independent of relatives treatment -coping and adaptation Social support -limited controlled research -relative excluded -reduce family burden, increase coping skills Psychoeducation -Duration-9m-2y -EE research -adjunctive to relatives treatment -behavioral management, family system, cognitive behavioral approach -extensive randomize controlled trials(RCTs) -Relative included -reduce relapse &increase functioning
EE Defined as criticism, hostility and emotional over evolvement of families
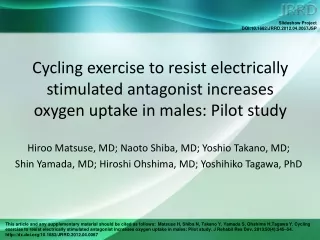
Effects of EE and medication on relapse in schizophrenia Bebbington and Kuipers, 1994
In most models the relative with a psychiatric disability is required to be in treatment . They have two primary objectives: providing informationregarding the disorder and its treatment and teaching strategies to cop with the illness, which include problem solving skills , coping and communication skills development , and crisis management .
Ultimately ,these objectives lead to the goals of improving the quality of life for both the family and relative with psychiatric disability , improving the functioning of the family as a unit , And reducing family environmental stress.
Positive Outcomes from FPE The patient and family work together towards recovery. Can be as beneficial in the recovery of schizophrenia and severe mood disorders as medication.
Outcome studies report a reduction in annual relapserates for medicated, community-based people of as much as 50%by using a variety of educational, supportive, and behavioral techniques.
Research with Family Psychoeducation • Functioning in the community improves steadily, especially for employment. • Family members have less stress, improved coping skills, greater satisfaction with caretaking and fewer physical illnesses over time.
Over 16 controlled clinical trials, comparing to standard outpatient treatment, have shown: Much lower relapse rates and rehospitalization Up to 75% reduction of rates in controls; minimally 50% -Increased employment At least twice the number of consumers employed, and up to four times greater--over 50%employed after two years--when combined with supported employment -Reduced negative symptoms, in multifamily groups -Improved family relationships and reduced friction and family burden -Reduced medical illness --Doctor visits for family members decreased by over 50% in one year, in multifamily groups
Family Psychoeducation This treatment is an elaboration of models developed by Anderson, Falloon, McFarlane, Goldstein and others.
MacFarlen intervention Combines two family psychoeducational interventions Family behavioral management And Multiple family approaches this is along term intervention with close membership
First stage practitioner meet individually Each family to build alliance and join with family Next stage is a work shop ,this model employs problem solving groups. . Thus families receive support and problem solving suggestions from another.
First year multifamily group focuses on social stabilization of patient. Second year group emphasize social and vocational rehabilitation for their ill relatives.
Family psychoeducation and multifamily groups: Basic techniques
Stages of a psychoeducational multifamily group Educa- tional workshop Ongoing MFG Families and patients 1-4 years Joining Family and patient separately 3-6 weeks Families only 1 day
Phases and Interventions in Family PsychoeducationYear One: Relapse Prevention • Engaging individual families • Multifamily educational workshop • Implementing family guidelines • Reducing stigma and shame • Lowering expectations • Controlling rate of recovery • Reducing intensity and exasperation
Phases and Interventions in Family PsychoeducationYear Two: Rehabilitation Gradually increasing responsibilities Moving one step at a time-- Monitoring encouragement from family members Establishing inter-family relationships Focusing family interests outside family Restoring family's natural social network
Structure of SessionsMultifamily groups (MFGs) and single-family treatment (SFT) MFG SFT 1. Socializing with families 15 m. 10 m. 2. A Go-around, reviewing-- 20 m. 15 m. a. The week's events b. Relevant biosocial information c. Applicable guidelines 3. Selection of a single problem 5 m. 5 m. 4. Formal Problem-solving 45 m. 25 m. a. Problem definition b. Generation of possible solutions c. Weighing pros and cons of each d. Selection of preferred solution e. Delineation of tasks and implementation 5. Socializing with families 5 m. 5 m. Total: 90 m. 60 m.
Rehabilitation effects of multifamily groups -Reducing family confusion and tension -Tuning and ratification of goals -Coordinating efforts of family, team, consumer and employer -Developing informal job leads and contacts -Cheerleading and guidance in early phases of working -Ongoing problem-solving -
Therapeutic processes in multifamily groups Stigma reversal Social network construction Communication improvement Crisis prevention Treatment adherence Anxiety and arousal reduction
انتخاب روش مداخله بستگی به زمان مداخله وضعیت زندگی و مراحل بیماری روانی دارد
مهارتهای مورد نیازبرای جلب نظر خانواده بیمار روانی مزمن و حمایت از آنها به منظور ارائه خدمت به بیمار هفت مورد می باشد :
اول: همکاری با خانواده دوم: ارائه اطلاعات لازم در مورد بیماری روانی مزمن به خانواده سوم: بهبود روابط خانواده و حل مشکلات چهارم: کمک به خانواده جهت استفاده از مراکز توانبخشی و درمان بیماران روانی مزمن وخدمات موجود پنجم: کمک به خانواده جهت رفع نیازها ششم: کمک به خانواده جهت روبرو شدن با حالات خاص بیماری روانی مزمن هفتم: توجه به حفظ اسرار
همكاري با خانواده مهارتها ي لازم ايجا بر خورد اوليه مثبت با خانواده . مصاحبه با خانواده براي گرفتن شرح حال ، نيازها ،تمايلات وتوانايهاي بيمار وخانواده . خانوادهايي كه به شيوه منفي به بيمارشان برخورد مي كنند (انتقادات خصمانه ) يا بيش از حد رفتاري ايثارگرانه دارند شناسايي كنید .
ارتباط مناسب مودبانه صحبت كردن ،خوب شنيدن وهمدلي در زمان درد ونااميدي خانواده . پيوند دادن تجربيات ومشاهدات خانواده ها با اطلاعاتي در مورد بيماري در زمان مناسب . آگاه كردن خانواده در باره خدمات شبانه روزي در شرايط استرس آور . برخورد مودبانه با اعضاي خانواده شامل توجه بدون تاخير به تماسهاي تلفني آنها .
آموزش و ارائه اطلاعات در خصوص بيماري رواني مهارتهاي لازم به سوالاتي كه خانواده در مورد بيماري رواني دارند،پاسخ دهيد . به خانواده كمك كنيد تا حالت متغيير وطولاني مدت بيماري را درك كند . گروههاي چند خانواده اي را تشكيل دهيد وراهنمايي كنيد . دسترسي به اين اطلاعات مي تواند به از بين رفتن سردر گميوكاهش استرس واضطراب و انگ بيماري رواني مزمن كمك مي كند
تشکیل گروه های چند خانواده ای بیماران روانی مزمن می تواند برای حمایت از خانواده و بیمار روانی مزمن و انگ زدایی از آنها راه خوبی باشد و انزوای خانواده که در نتیجه بیزاری و احساس گناه خانواده از حضور بیمار روانی مزمن در خانواده است از بین خواهد رفت.
با معرفي كردن اختلال رواني به عنوان يك بيماري مغزي وابسته به فشارهاي رواني مي توانيد به كاهش احساس ناكامي خانواده واحساس رنجش به بيمار كمك كنيد . 1- صادق باشيد. 2- اطلاعات را بر اساس ارزيابي دقيق نيازهاي خانواده ارائه كنيد. 3- منطبق با سطح فهم خانواده گفتگو كنيد . 4- تبادل اطلاعات ومهارتها را بين اعضاي خانواده تشويق نمائيد .
افزايش مهارتهاي خانواده براي برقراري ارتباط وحل مشكل مهارتهاي ارتباطي افزايش آگاهي هر فرد از رفتارهاي تطابقي وخوشايند وتاييد آن با ارائه پسخوراند مثبت به ساير اعضاي خانواده . به كارگيري فعالانه مهارتهاي شنيداري . بيان درخواستهاي مثبت . بهتعرين زمان آموزش مهارتاي ارتباطي هنگامي است كه بيمار در بهبودي نسبي مي باشد .
پندهاي مهم به خانواده در اين دنيا همه چيز تغيير ميكند- -شما در دوي استقامت شركت كرده ايد نه در يك دوي سرعت ،كاهش علائم بيماري رواني مزمن نيازمند يك دوره طولاني است . پيشرفت آهسته سريعترين راه بهبود است .- -مشاركت سا لم خانواده فراز ونشيب دارد .هيچ كسي هميشه در اوج نيست .