Download
1 / 13
130 likes | 270 Views
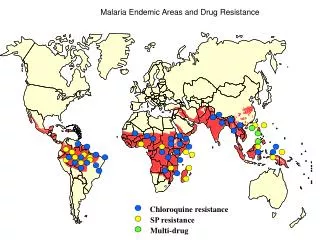
Frameworks and Processes for malaria control, drug quality and artemisinin resistance in Asia. Why discuss frameworks and processes ?.

E N D
Frameworks and Processes for malaria control, drug quality and artemisinin resistance in Asia
Whydiscussframeworksandprocesses? • Protection of drug efficacy a global concern, but also essential for Asia’s growth and prosperity. Malaria may even experience resurgeancein countries where it has almost been eliminated. • Individuals with fever need effective medicine, but efficacy is undermined by poor quality and outright counterfeiting. • Drug producers in this region will lose substantial investments if their products no longer work. • The frameworks, processes and programs to be discussed here reflect the global and regional response. Is it as strong as it should be, or can APLMA help make it more effective?
What hasbeendonesofar? • Global concern about antimicrobial resistance – tuberculosis, bacterial infections, malaria • WHO has set guidelines and certification procedures for Good Manufacturing Practices (GMP); Global Fund and PMI require pre-qualification of suppliers. • National regulatory authorities license medicines, authorize imports, test pharmaceutical products in the market. • Regional and global organizations share information, standardize processes, and build capacity.
What are some of the key organizations and programs? • WHO and the Emergency Response to Artemisinin Resistance (ERAR) provide overall guidance • ASEAN working groups standardize definitions and regulations • National regulatory authorities issue licenses and test drugs • United States Pharmacopeia builds national and regional capacity • BREMERE shares information within and between national programs • Malaria Medicine Regulators develop strategies for licensing and regulating related pharmaceutical products.
Aretheseeffortsworking? • We are starting fast now, but time is short and we have much to do. Leadership and strong field implementation will continue to be essential. • Artemisininresistance is being documented in many new places and will become more evident as non-resistant parasites are eliminated. • ERAR and APLMA convey recognition of urgency and have already had an impact. • Global Fund has inserted new financial resources, but gaps remain and GF is often not an easy partner.
Here’s the challenge? Is it quality?effortsworking? • We are starting fast now, but time is short and we have much to do. • Artemisinin resistance is being documented in many new places and will become more evident as non-resistant parasites are eliminated. • ERAR and APLMA are markers of urgency and have already had an impact. • Global Fund has inserted new financial resources.
But why are we concerned? What are the problems? • Money and commodities may be more abundant, but absorption capacity hasn’t kept up. • Both technical and human resources are inadequate. • Resources tend to be compartmentalized, for use within individual countries and projects, making organizational sustainability and inter-country activities difficult. • We still haven’t figured out how to ensure good case management and follow up in the mobile populations at greatest. • The multiple private sectors – drug producers and distributors, clinicians, organized and informal employers – are not fully engaged and may not share framework objectives. • SSFFC (Substandard/Spurious/Falsely-Labelled/Falsified/Counterfeit) drugs are still in use and contribute directly to resistance. • Consumer and retailer understanding of drug quality is deficient.
What can we do? 1: Engage with all interested groups to broaden “ownership” • Artemisinin resistance partly driven by broad economic, political and sociological factors, but our frameworks and programs primarily reflect public health interests and approaches. • Collaborate with efforts to control anti-microbial resistance (TB, antibiotics). • Identify and incorporate legitimate private sector concerns. • Use disease control approaches to support business development. • Engage “all-of-government” (military, commerce, police, etc.)
What can we do? 2: Encourage strategies that focus on drug movements and people-at-risk, rather than on political boundaries and projects • The frameworks and programs discussed earlier recognize that artemisinin resistance is a regional problem and a global threat. Fragmented responses are inefficient and potentially ineffective. • Use process improvement techniques to simplify and expedite drug procurement, importation, inspection, testing and distribution. • Ask donors to facilitate strategies that focus on inter-country migrant corridors.
What can we do? 3: Support recommendations of Malaria Medicine Regulators • Establish fast-track regulatory approval to increase availability of fixed dose combination formulations, to improve patient compliance and provide flexibility for addressing changes in antimalarial resistance. • Implement communication initiatives to improve quality use of antimalarials. • Strengthen regional collaboration between NRAs to build capacity and increased convergence of good regulatory practices • NRAs to more pro-actively work with other government agencies, malaria control programs and stakeholders, recognising the particular vulnerability of mobile and remote populations and the prevalence of artemesinin resistance in border regions.
What can we do? 4: Strengthen shared regional capacity and encourage national regulatory authorities to share resources • Continue efforts to standardize processes and strengthen regional organizations. • Develop shared regional resources for quality and efficacy testing. • Approach donors for “non-projectized” organizational development resources, including human capacity and equipment.
Headline HereConsecteturadipiscingelit. Phasellusodioleo, ornare in vulputateullamcorper, pellentesque sit ametlectus. Fusce a veliteuauguetemporcongue in quisodio. Cras ac nibhutipsumsempervehicula. Nuncblanditmattisinterdum. Sedlaciniaadipiscingnisl. Nam velnullasapien, egetplaceratturpis. Duis et commodoerat. Vivamus quam urna, consequat at tempor a, lobortis ac purus.