Download
1 / 34
360 likes | 748 Views
Management of the Partial Foot Amputee. Gait Workshop at Biomechanics Laboratory, U of Sydney July 2005. 3.2.2 SURGICAL GOALS

E N D
Management of the Partial Foot Amputee Gait Workshop at Biomechanics Laboratory, U of Sydney July 2005
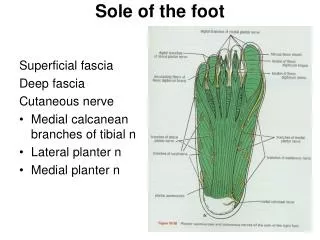
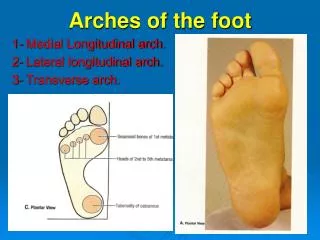
3.2.2 SURGICAL GOALS • 'To remove the pathologic condition which interferes with function, causes disability or threatens life so that rehabilitation can be instituted' (Mueller and Sinacore, 1994). Figure 1 - Lines of standard forefoot/midfoot amputations (From Vitali, et al., 1978, pp. 128).
Biomechanical Complications • www.gentili.net.amputations • An equinus deformity often results from forefoot amputations, especially the Lisfranc (metatarsocuneiform joint) and the Chopart (talonavicular and calcaneocubiod joints) amputation (Chang, et al., 1995). • In a TMA the tendons of extensor hallucis longus, extensor digitorum longus and peroneus tertius muscles are sectioned. These muscles act to dorsiflex the foot at the ankle, if they are sectioned, an imbalance between the anterior and posterior muscle groups exists. This leads to the Achilles tendon working unopposed, thus creating an equinus deformity (Barry, et al., 1993). To overcome this, an Achilles tendon lengthening procedure is performed. • This loss of dorsiflexion range of motion can lead to excessive loading at the distal edge of the residuum during gait and lead to skin breakdown (Chang, et al., 1994).
3.2.5 SURGICAL TECHNIQUE The following surgical technique is summarised from Gregory, Peters and Harkless, 1992. Figure 5 illustrates a transmetatarsal amputation procedure. Figure 5 - Transmetatarsal amputation procedure (From Sanders, 1986, pp. 102).
Partial Foot Gait Dr Michael Dillon Clinical observation suggests • Residuum rotates within shoe/prosthesis • Prostheses do not have a socket • Prostheses do not have a stiff toe lever • Triceps surae atrophy • Reduced plantarflexion • Amputees can’t stand on their toes
Literature suggests • Prostheses restore the lost foot length or lever-arm (Condie 1970, Rubin 1984, Pullen 1987, Stills 1987, Weber 1991, Mueller and Sinacore 1994, Saunders 1997, Sobel 2000) • Function is improved by maintaining residual foot length and ankle motion (Wagner 1985, Mueller et al1986, Barry etal 1993, Helm 1994, Pinzur at al 1997, Sobel 2000) • MYTHS??
Method • Amputee subjects (n=8), • 5 unilat (TMT, Lisfranc, Chopart) • 3 bilat (MTP, Lisfranc, Chopart) • Aetiology: trauma or gangrene • Normal subjects (n=8), age, ht, wt, sex matched • Apparatus: Peak Motus 3D motion analysis system, AMTI force platform
For all conditions the motion is biased towards DF. The forefoot should contribute 10 degrees of plantarflexion relative to rearfoot. There is none in barefoot PFA in preparation for toe-off and closer to normal with boot and CTO. Knee is held at >10 degrees F throughout the gait cycle. Knee F is delayed, amplitude diminished in barefoot. Over stance phase the hip moved from a flexed position to extended position, and returns to flexion during swing phase. Amplitude is diminished in barefoot. Partial Foot Gait
Moment • Is the rotational version of force. It is the turning effect around the centre of rotation. It is generated by muscles or an external force acting on the segment. Magnitude of a moment depends on size of the force and the distance from the centre of rotation. (Newton.metres)
Partial Foot Gait • Ankle moment in barefoot is toward plantarflexion throughout stance. VGRF vector remained posterior to the ankle joint centre. • Traditional and CTO bring ankle jt moment in sagittal plane closer to normal, but only at 30% stance. • Knee has F moment to 20% stance, E moment to 50% stance, F moment again to 80%, then E to toe off. Boot is more normal, CTO is further towards normal. • Hip has extensor moment in first half of stance and flexor in the second half. Moments increase from barefoot to Traditional to CTO. F moment in barefoot is delayed to after toe-off, but before toe-off for traditional and CTO.
Power • Is the rate at which work is done. The moment multiplied by the angular velocity of the joint. The area under the power curve is the work done for that period.
Joint Power • Is an indication of how hard the muscles around that joint are working. • Is the rate at which energy is expended or absorbed • Area under the graph • Negative power means muscles are absorbing energy. • Positive power means energy is generated by the muscles around the joint.
Partial Foot Gait • In barefoot, ankle jt power is (+) generating from 20 – 90% of stance. The traditional has periods of absorption and generation. CTO has large absorbing periods early in stance and generation prior to toe-off. • Knee jt powers are near normal. • Hip jt power have increasing amounts in traditional and CTO.
Results • Once the MT heads had been amputated, the GRF did not continue to progress distally along the length of the residuum but remained well behind the distal end throughout most of stance phase • In the TMT and Lisfranc Amputees fitted with toe fillers, foot orthoses or slipper sockets, the distal end of the residuum was located at 58-65% of shoe length. • The largest VGRF occurred at 45% of the gait cycle and did not progress past the distal end of the residuum until after contralateral heel contact in double limb support.
Significant reduction in peak power generation across the ankle were observed on the affected limbs of all amputees except the bilat MTP amp. • Bilat MTP amp: small reductions in power generation, COP excursion, but not joint angular velocity or ankle ROM. • TMT amp: power generation 0.72W/kg • Lisfranc amp: power generation 0.91W/kg • Chopart amp: 0.78W/kg (unilat), 0.32W/kg (bilat) due to elimination of joint range rather than COP. • Normal: 2.56 to 5.06W/kg • Reduced due to diminished ankle moment coupled with reduced joint angular velocity.
Results • Reductions in work across the affected ankles were compensated for by increased power generation at the hip joint (ipsilateral or contralateral). The kinetic patterns observed were variable.
Results • In the Chopart amputees fitted with clamshell devices demonstrated the COP was able to progress well beyond the distal end of the residual limb shoe length commensurate with the 2nd peak VGRF.
Discussion • The COP remained proximal to the distal end of the residuum until contralateral heel contact • It is difficult to determine why these amputees adopted this gait pattern • Spare the distal residuum from extreme forces • Reduce the requirement of the triceps surae • Toe fillers, foot orthoses, AFOs and slipper sockets seemed unable to restore the ‘effective’ foot length • The clamshell PTB prosthesis incorporated a substantial socket • Toe levers were made from carbon fibre plates or prosthetic feet
Discussion • One of the primary functions of the ankle is to generate power necessary to walk. • Once the metatarsal heads were affected, power generation was negligible irrespective of residual foot length • Lisfranc and TMT amputees, performed as much work across the ankle as did the Chopart amputees who had no ankle motion. • The primary reason for partial foot amputation is to capitalize on the ankle’s contribution to walking. • There is little benefit to be gained by striving to maintain residual foot length and ankle motion.
Discussion • Once amputation has compromised the metatarsal heads, maintaining foot length should no longer be the primary surgical objective. • Aim for residuum that has good distal skin coverage and primary intention healing. • Given that the ankle did not contribute greatly to the work required to walk and the likelihood of complications with fitting most amputees, abandon below ankle designs and go for a clamshell design where risks are minimized.
Conclusion • Gait analysis on ‘normals’ provided foundation for our understanding of PFA • Gait analysis was used to provide more accurate description of gait and prosthetic fitting. • Insights from gait analysis challenged misconceptions and forced reflection on clinical practice • Improved understanding of what didn’t work has led clinicians to pursue advancements in design.