Download
1 / 21
210 likes | 396 Views
CHAPTER 14. Psychological Disorders Affective Disorders. Affective Disorders. Affective disorders Disorder of mood Include depression, bipolar disorder, mania Any disorder of affect Disorder must be relatively enduring Not a change in “mood” per se, but change in ability to regulate mood

E N D
CHAPTER 14 Psychological Disorders Affective Disorders
Affective Disorders • Affective disorders • Disorder of mood • Include depression, bipolar disorder, mania • Any disorder of affect • Disorder must be relatively enduring • Not a change in “mood” per se, but change in ability to regulate mood • Disturbance must last for several months • Set of criteria for each disorder • Emerging question: with available pharmaceuticals, are we over-diagnosing “depression” for normal mood changes?
depression • Major depression • person often feels sad • But extreme: • hopelessness for weeks at a time • loss of the ability to enjoy life • Disturbances in relationships and sexual interest • loss of energy and appetite • slowness of thought • sleep disturbance. • In some cases the person is also agitated or restless. • Stress is often a contributing factor, but major depression can occur for no apparent reason. • Depression may appear alone as unipolar depression, or depression and mania may occur together in bipolar disorder.
mania • Mania involves • excess energy and confidence • often leads to grandiose schemes. • Typically laos involves • Decreased need to sleep, • increased sexual drive, • Often, abuse of drugs or alcohol • Mania may also appear alone as unipolar mania, or depression and mania may occur together in bipolar disorder.
Affective Disorders • Bipolar disorder • the individual alternates between periods of depression and mania. • Mania can occur without periods of depression, but this is rare. • Bipolar patients often show psychotic symptoms • Delusions • Hallucinations • Paranoia • Other bizarre behavior. • Incidence rate is fairly high: 4.4% of population in U.S. • http://www.youtube.com/watch?v=9ZnAG38CWZI
Bipolar subtypes • Bipolar I: individual has experienced one or more manic episodes with or without major depressive episodes. • Bipolar II • characterized by hypomanic episodes rather than actual manic episodes • at least one major depressive episode • There has never been a full manic or mixed episode. • Hypomanic episodes do not go to the full extremes of mania (i.e. do not usually cause severe social or occupational impairment, and without psychosis • makes Bipolar II more difficult to diagnose, • For both Bipolar I and II: number of specifiers that indicate the presentation and course of the disorder, • chronic, • rapid cycling • catatonic • melancholic
Bipolar subtypes • Cyclothymia • involves a presence or history of hypomanic episodes with periods of depression that not meet criteria for major depressive episodes • Requires presence of numerous hypomanic episodes intermingled with depressive episodes • Again do not meet full criteria for major depressive episodes. • low-grade cycling of mood which appears to the observer as a personality trait, but interferes with functioning. • Bipolar NOS • Rapid cycling • Most people who meet criteria for bipolar disorder experience a average of 0.4 to 0.7 cycles per year, lasting three to six months • defined as having four or more episodes per year • found in a significant fraction of individuals with bipolar disorder.
Incidence of affective disorders • 1 in 5 people (20% of population) will suffer a true mood disorder in their lifetime, most likely depression. • Women are 2-3x more likely than men to suffer from unipolar depression during their lifetime • May be social/reporting issue however • Women more likely to report symptoms than men • . • Bipolar illness occurs equally often in both sexes: about 4%. • Risk • The risk for major depression increases with age in men, • Women experience peak risk between the ages of 35 and 45. • Greatest risk for bipolar disorder: early 20s to around age 30.
Heritability? • Depression shows fairly high heritability • When one identical twin has an affective disorder, probability the other twin will have illness as well is about 69%, • Only 3% in fraternal twins. • Mania: Heritability is somewhere around .37 • number somewhat higher for women than for men • Again, may be reportability issue. • Bipolar disorder is more heritable, with recent estimates of .85 and .93.
Treatment of Affective Disorders • One of first antidepressants = Iproniazid • introduced as a treatment for tuberculosis • discovered that the drug produced elevation of mood and was an effective antidepressant. • Iproniazid increases activity at monoamine receptors • Remember: monoamine receptors = dopamine, norepinephrine, and serotonin • Led researchers to the monoamine hypothesis • depression involved reduced activity at norepinephrine and serotonin synapses.
Drug treatments • All effective antidepressant drugs increase activity of norepinephrine and serotonin, or both, at the synapses. • MAO inhibitors: monoamine oxidase inhibitors • block the destruction of excess monoamines in the terminals • Include Parnate (tranylcypromine sulfate) and Nardil (phenelzine sulfate • tricyclic antidepressants • block reuptake at the synapse • Include Elavil (amytriptaline), amitriptyline, ortriptyline, doxepin and desipramine
Drug treatments • Second-generation antidepressants • affect a single neurotransmitter or set of neurotransmitters • E.g., SSRIs, serotonin selective reuptake inhibitors • SNRIs: norepinephrine selective reuptake inhibitors • For example, Prozac (fluoxetine); Lexapro, Effexor • These synaptic effects occur within hours, but symptom improvement takes two to three weeks. • Some significant side effects • Weight loss/gain • Sexual side effects
Non-drug treatment • Electroconvulsive therapy (ECT) • involves applying 70 to 130 volts of electricity to the head of an anesthetized patient, • produces a seizure and convulsions. • Essentially CONTROL-ALT-DELETE • http://www.youtube.com/watch?v=zYl13Relzbs • Without the seizure activity in the brain that produces the convulsions, the treatment does not work. • ECT : usually reserved for patients who • do not respond to the medications • who cannot take them due to extreme side effects or because of pregnancy. • Like drugs, ECT increases sensitivity of postsynaptic serotonin receptors. • Produces reduction in sensitivity of autoreceptors on the terminals of norepinephrine- and dopamine-releasing neurons • Result is increased release of those transmitters is increased.
Other issues occuring with Affective Disorders • Changes in circadian rhythm • Circadian rhythm: day/light regulatory cycle • Slightly long than 24 hours • – tends to be phase advanced in affective disorder patients. • Patients with depression enter rapid eye movement sleep (REM) earlier in the night and spend more time in REM than normal. • Alternative treatment: change circadian rhythm • Some patients who unresponsive to medication get relief from depression by readjusting their circadian rhythm. • Some depressed patients also benefit from reducing time in REM sleep.
Seasonal-Affective Disorders • Seasonal Affective Disorder(SAD). • Some people’s depression rises and falls with the seasons: known as SAD • Most SAD patients more depressed during fall /winter, • improve in spring and summer. • Smaller number experience depression in the summer and improve in the winter. • What about Southern hemisphere? • Depression worse in June, July, August • Their winter! • Treatment for SAD: Phototherapy • sit in front of high-intensity lights for couple of hours or more a day. • Why? Resets circadian rhythm, increases melatonin • Suggests that depression tied to circadian rhythm
Treatment for bipolar Disorders • Lithium • metal administered in the form of lithium carbonate • Typically the medication of choice for bipolar illness. • It is most effective during the manic phase • also prevents further depressive episodes. • Why? • most likely stabilizes neurotransmitter and receptor systems • prevents the large swings seen in manic-depressive cycling.
Treatment for bipolar Disorders • Anticonvulsant medications • Generally decrease likelihood of action potential • Next best medication of choice for bipolar illness. • Include gabapentin (Neurontin), zonisamide (Zonegran) and topiramate (Topamax); Tegretol, etc. • Again, works best for manic episodes • also prevents further depressive episodes. • Works for similar reasons as lithium • What about antidepressants for bipolar? • Generally contraindicated • Why? May kick start manic episode • If used, under careful watchful eye of physician/psychologists
Brain changes in Affective Disorders • Affective disorders are associated with structural abnormalities in several brain areas. • Much like schizophrenia, but slightly different brain areas • Volume deficits in hippocampus, prefrontal areas • especially the dorsolateral cortex and subgenual prefrontal cortex. • The amygdala is increased in volume. • All these structural alterations are accompanied by changes in activity level. • In most cases, affective disorders are not as debilitating as schizophrenia • Most individuals respond well to treatment • Must change social/life coping skills to prevent relapse • Only very small percentage is treatment-resistant
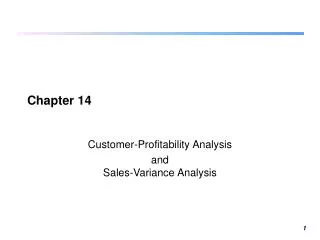
Blood flow was decreased (a) in the caudate nucleus and (b) in the dorsolateral prefrontal cortex (where the arrows point). The color scale is reversed in the scan in (a); yellow and red in that image indicate decreased activity.
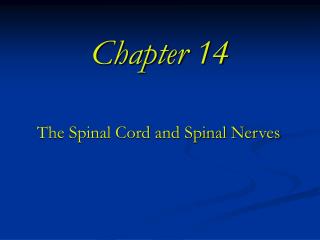
Increased activity in the ventral prefrontal cortex and amygdala in depression
Brain changes in Affective Disorders • In most cases, affective disorders are not as debilitating as schizophrenia • Most individuals respond well to treatment • Must change social/life coping skills to prevent relapse • Most effective therapy: • Initially drug treatment + cognitive behavioral therapy • Cognitive behavioral therapy may be sufficient if no crisis • Only very small percentage is treatment-resistant