Download
1 / 27
380 likes | 1.64k Views
Hypokalemia-causes. Decreased K intake Low calorie diets – rare Increased K entry into cells Alkalosis Increased insulin Increased Catecholamines Channelopathies Increased RBC production Hypothermia Chlorquine intox. Hypokalemia. Increased GI losses

E N D
Hypokalemia-causes • Decreased K intake • Low calorie diets – rare • Increased K entry into cells • Alkalosis • Increased insulin • Increased Catecholamines • Channelopathies • Increased RBC production • Hypothermia • Chlorquine intox
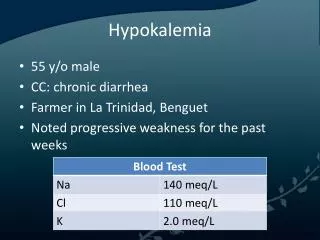
Hypokalemia • Increased GI losses • Vomiting, Diarrhea, NG tube, laxatives • Increased Urinary losses • Diuretics • Mineralocorticoid excess • Nonreabsorbable ions • Metabolic acidosis • HypoMg • Nephropathies • Ampho B • Polyuria • Licorice
Hypokalemia • Increased Sweat Losses • Dialysis • Plasmaphoresis
Presentation • Neuro muscular K 2-2.5 • Weakness prox > distal, loss of reflexes • Cardiac • Arrhythmias • EKG • U waves, prolonged QT, small T wave Hyper K+ T wave Hypo K+ K+ K+ K+ K+ K+ K+ K+ K+
Familial Periodic Paralysis • Types • Hyper Kalemic – HyperPP • Hypo Kalemic – HypoPP • Thyrotoxic- TPP • Genetic mutation • Autosomal dominant and sporadic
Channelopathies • Inability to find a decent TV program despite having cable and 150 channels to chose from. • Functional disturbances of ion channels in the cell membrane • “Flaccid muscle weakness due to under excitability of sarcolemma.”
HypoPP • Rare, potentially fatal episodes of muscle weakness • Asian population • Acute attacks due to K+ moving into cells • Precipitated by exercise, carbs, stress • K level • Low • Normal* (low K + Rhabdo) • Often self limiting
Treating K problems • ABCs • IV – O2 – Monitor • Stat labs • Check Mg, CPK, TFTs • Oral K is good for non life threatening hypoK • Watch N/V • Use PO KCl if hypo K is due to loss of Cl
HypoPP - Rx • Administer K+ • 10-20meq/hr IV (Higher via central line if severe) • 40-60meq PO x2 • Check the K+ q 15-30min • Rx thyrotoxicosis w/ propanolol
HypoPP - Discharge • Daily oral K does not prevent attacks • Carbonic anhydrase inhibitors- Acetozolamide • Low carb diet • Consult/referral
Caveats – K problems • 1meq decrease in K represents 300meq deficit* • If hypo K is due to loss • Remember, 98% of K is in the ICF • 0.1 drop in pH raises K by 0.6 • Think of acid/base problems • Is this primary or secondary problem?
Dangers in Rx PP • Check the type before starting K • Must confirm if hypo, hyper or nl • Remember this is a cellular shift • Rebound hyper K can occur if you are too aggressive w/ K replacement • Watch for respiratory insufficiency !
M U D P I L E S • Methanol/Ethylene glycol • Certainly possible • Pt denied • No visual sx • No Ca oxalate xtals • Woods lamp • Osm gap
M U D PI L E S • Uremia • BUN/Creat OK • DKA • Not a diabetic, Glucose OK • Paraldahyde • No pungent odor • Isoniazid • No hx TB Rx
M U D PIL E S • Lactic Acidosis • Abd pain -> dead gut • Decreased perfusion • Liver failure • Alcohols • Meds • Inborn errors • Lactate -> 27
M U D PILE S • Ethanol - Alcohol Ketoacidosis • Binge drinker, Not eating • Salicylates • No Hx of ASA use
Hospital Course • Developed DTs • + C. Dif culture • Feeding tube placed • acute alcoholic hepatitis and severe dehydration and metabolic disarray with severe hypokalemia, hypophosphatemia, hypomagnesemia, acute renal failure, lactic acidosis,
Alcohol ketoacidosis • Uncommon, often missed • Binge drinkers
AKA - 3 factors • Alcohol intake • Decreased caloric intake • Volume depletion Results in starvation physiology
AKA • Decreased caloric intake • Counter regulatory hormone release • Epinephrine, cortisol, growth hormone • Elevated glucagon, decreased insulin • Promotes lipolysis and fatty acid mobilization • Volume depletion • Elevated glucagon, decreased insulin
AKA • Alcohol intake • Oxidation of ETOH-> ->acetate • NAD->NADH which raises glucagon, decreases insulin • Promotes betahydoxybutyrate vs acetoacetate • Decreased gluconeogenisis
AKA • Symptoms • N, V, abd pain • Dyspnea, tremulousness • Muscle pain, fever, diarrhea, syncope, Sz • Physical • Tacycardia, tachypnea, abdominal pain, • Hepatomegaly, hypotension
AKA • Differential Dx • Cholecystitis • Peptic ulcer, gastritis • Mesenteric ischemia • Pacreatitis • Withdrawal syndromes • Metabolic acidosis • DKA • Methanol, Ethylene glycol
AKA - labs • pH –low, high or nl • Metabolic acidosis -> ketones • Metabolic alkalosis -> vomiting • Respiratory alkalosis -> hyperventilation • Serum ketones low, high or nl • Betahydoxybutyrate • Lytes –abnormal • Lactate – mildly elevated
AKA-treatment • Volume replace • Carbohydrate replacement • D5NS • Fix electrolyte abnormalities • K, Mg, acidosis • Address associated problems • Withdrawal, Wernikes, GI bleed, hepatitis, pancreatitis, pneumonia, rhabdo, etc.
I have never been lost, but I will admit to being confused for several weeks.