Download
1 / 85
850 likes | 995 Views
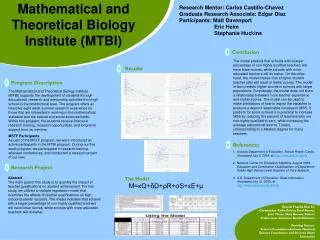
Issues in MTBI. Ford Vox, MD Staff Physician, Shepherd Center, Brain Injury Rehabilitation Program Adjunct Assistant Professor, Emory University School of Medicine. Today's Topics. The debate: mTBI/Concussion as a major cause of disability Pro / Con. Traumatically induced physiological

E N D
Issues in MTBI Ford Vox, MD Staff Physician, Shepherd Center, Brain Injury Rehabilitation Program Adjunct Assistant Professor, Emory University School of Medicine
Today's Topics • The debate: mTBI/Concussion as a major cause of disability • Pro / Con
Traumatically induced physiological disruption of brain function, as manifested by at least one of the Following: 1) Any period of loss of consciousness. 2) Any loss of memory for events immediately before or after the Accident. 3) Any alteration in mental state at the time of the accident (eg, feeling dazed, disoriented, or confused). 4) Focal neurological deficit(s) that may or may not be transient. AND *Loss of consciousness of approximately 30minutes or less. *After 30minutes, an initial Glasgow Coma Scale (GCS) score of 13–15. * and posttraumatic amnesia (PTA) not greater than 24 hours. ACRM Definition of MTBI
1) Direct blow to the head, face, neck, or elsewhere on the body with an "impulsive" force transmitted to the head 2) Rapid onset of short-lived impairment of neurological function that resolves spontaneously. 3) Acute clinical symptoms primarily reflecting functional disturbance versus structural injury. 4) Graded set of clinical syndromes that may or may not involve loss of consciousness (LOC), with resolution of clinical and cognitive symptoms generally following a sequential course. 5) Typically grossly normal structural neuroimaging studies. International Conference on Concussion in Sport
MTBI Pathophysiology: DAI Axonal stretching Pathological excitatory neurotransmitter release. Disruption of ion gradients Metabolic mismatch / vulnerability Increased glucose demand to feed Na/K pump No change in CBF Normalization: days to weeks. Giza & Hovda 2001
Proposition: MTBI Disability is Overblown
Proposition: MTBI is a Major Cause of Disability
An Ordinary Football Game, Then a Player Dies October 19, 2011 “Concussion” mentioned 5X in the article Subdural hematoma = Not a concussion
An Ordinary Football Game, Then a Player Dies October 19, 2011 “As those who play and coach football learn new ways to improve safety — through training, medical response and equipment — sometimes they are left to contemplate this: brains remain vulnerable, and even the most ordinary collisions on the field can kill.”
Alarming numbers: 1.7 Million/year (CDC ER data) 1.4 - 3.8 Million/year (Comprehensive) Need for public ed: belief LOC required still widely held. Point: Media right to alarm
Catastrophic injury: Second Impact Syndrome Teenagers Malignant brain swelling Second hit during symptomatic period 94 Cases from 1989-2002 - 75 SDH, 10 SDH with diffuse swelling, 5 diffuse swelling, 4 AVM or aneurysm - 92 cases high school (2 college) - 59% previous concussion(s). - 71% same season as death. - 39% evidence of residual symptoms from prior concussion. Point: Media right to alarm Boden AJSM 2007
Point: MTBI treatment suggestsa heterogeneous condition • Just as there is no unique PCS symptom, there is no unique treatment. • We tackle headaches, dizziness, sleep, etc, in their own treatment algorithms • Powerful treatment: Education: natural history, sleep hygiene, coping strategies, stress management, avoidance ETOH/drugs. Ponsford. Impact of early intervention on outcome following mild head injury in adults. J Neurol Neurosurg Psychiatry. 2002 Sep;73(3):330-2.
Symptoms complexes appear tied together. Require interdisciplinary treatment. Holistic approach. Point: PCS treatment should be patient-centered
CASE: A 34-year-old male MTBI patient complained of problems with attention and concentration. The medical records included documentation of cervical pain. When asked about his neck pain, the patient explained that turning his head during the night resulted in sharp pain that woke him up multiple times each night. At the time of the evaluation, this sleep disturbance had persisted for 4 months. His reduced mental stamina resulted in significant problems at work and he was placed on sick leave 3 weeks earlier. The combination of pain and reduced concentration resulted in an elevated stress level that further compounded the disordered sleep and pain cycle. Jogging was too painful, and thus his premorbid coping strategy for stress management was unavailable. The unrelenting high levels of stress resulted in tension headaches that originated in the back of his head and exacerbated his neck pain. This dysfunctional loop was self-reinforcing and not responsive to various medications that were prescribed. Ruff 2005
Clinical Practice Guidelines are of poor quality Rigor of development Editorial independence Little guidance for cases that do not remit spontaneously Point: Even the experts can't agree Quality of clinical practice guidelines for persons who have sustained mild traumatic brain injury. Brain Injury, July 2011; 25(7–8): 742–751
Can't lump together normals and the “Miserable Minority” One group says little about the other. Studies should focus on PCS population, not MTBI in general. Prediction of PCS should be the goal. Current factors crude, inflexible (age, gender, previous concussions, psych history, migraine history) Point: Need to study right signal
The acute symptoms and chronic symptoms are reflective of two distinct disorders Early symptoms have specific treatments (neurologic or psychologic). Early symptoms resolve. For patients that experience chronic symptoms, psychological factors dominate. The symptoms of chronic PCS can be seen after any trauma. There is no need for a TBI. Point: PCS is meaningless
PCS prevalence after MTBI ranges from 10 to 64% depending on criteria used (ICD-10, DSM-IV, Rivermead) Studies of incidence rarely account for preinjury factors or include a proper comparison group Once numbers of everyone “dazed and confused” included, and “complicated” MTBI excluded, incidence drops to around 5%. Point: PCS is meaningless
PCS symptoms overlap with: Chronic pain Depression PTSD Healthy people PCS is a label that serves mask other conditions the clinician might diagnose and treat. Point: PCS is meaningless
Symptom checklist given to 1,116 Kaiser Permanente patients. Fox DD, Lees-Haley PR, Earnest K, Dolezal-Wood S. Base rates of postconcussive symptoms in health maintenance organization patients and controls. Neuropsychology 1995;9:606-611.
104 healthy volunteers in Vancouver. All had no history of psychological disorder, neurological disorder, or substance abuse. All given the British Columbia Postconcussion Symptom Inventory-Short Form Symptoms rated on Likert scale of intensity 79.6% met DSM-IV criteria, 72.1% met ICD-10 criteria Iverson GL, Lange RT. Examination of "postconcussion-like" symptoms in a healthy sample. Appl Neuropsychol 10:137–144, 2003
Memory Impairment: A Symptom of Life Things We Normally Forget "Symptom" Percent of People Forgets telephone numbers 58% Forgets people's names 48% Forgets where car was parked 32% Loses car keys 31% Forgets groceries 28% Forgets why they entered a room 27% Forgets directions 24% Forgets appointment dales 20% Forgets store location in shopping center 20% Loses items around the house 17% Loses wallet or pocketbook 17% Forgets content of daily conversations 17%
At least this part of Rick Perry is normal.
Athletic MTBI story casts doubt on general population's experience
80% of athletes have no symptoms at 3 weeks. Up to 80% of general population reports symptoms at 3 MONTHS. Can an athlete's physiology really be so different? Point: Too much variance with athletic MTBI Collins M, Lovell MR, Iverson GL, Ide T, Maroon J. Examining concussion rates and return to play in high school football players wearing newer helmet technology: A three-year prospective cohort study. Neurosurgery 2006;58:275-286. Sigurdardottir S, Andelic N, Roe C, et al. Post-concussion symptoms after traumatic brain injury at 3 and 12 months post-injury: A prospective study. Brain Inj 2009;23:489-497.
No similar dichotomy in pain/disability/recovery rates with musculoskeletal injuries. Torn ACL recovery similar in sports and general population Massive fudge factor – non-biological Athletes with long recovery times have early fogginess, memory deficit, or dizziness. General population: early anxiety predictive. Point: Too much variance with athletic MTBI Dischinger PC, Rybe GE, Kufera JA, Auman KM. Early predictors of postconcussive syndrome in a population of trauma patients with mild traumatic brain injury. J Trauma 2009;66:289-296.
Sports concussions: Population is more homogeneous: younger, healthier, more motivated. Circumstances: Acute stress reaction. Role of anticipation of the hit, mental readiness Non-athletic MTBI's: assaults, accidents, traumatic situations. Point: Athletic Advantage
Control: 223 volunteers, no history of head injury, and didn't know anyone with head injury. Comparison: 100 MTBI patients 1 to 7 years out referred to neuropsychology. Both groups asked to estimate the presence of 30 symptoms before and after an imaginary (control) or real (comparison) head injury. Point: Expectation becomes etiology Mittenberg W, DiGiulio DV, Perrin S, Bass AE. Symptoms following mild head injury: Expectation as aetiology. J Neurol Neurosurg Psychiatry 1992;55:200-204.
Little difference between what we expect to experience, and what we do • When symptoms rank ordered, correlation is 0.82. • Anticipated symptoms explain 67% of the variance in incidence.
MTBI patients underestimate normal rate of symptoms • Pattern suggests misattribution of symptoms to the MTBI.
Point: Expectation becomes etiology • Mittenberg Pathway: • 1) Activation of typical symptom expectancies when mild head injury occurs. The concussion is inherently stressful and also normally induces autonomic/emotional arousal • 2) Symptom expectancies bias selective attention to internal state • 3) Attentional bias and arousal augment symptom perception • 4) which then elicits additional autonomic/emotional response, reinforcing expectations.
Medical Student's Disease 70% of medical students express concern about their own symptoms and sensations matching diseases they have learned about. On spectrum of hypochondriasis