Download
1 / 28
300 likes | 508 Views
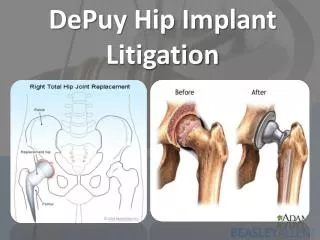
Case Study. Early Failure of a Modular Hip Implant. Summary of Failed S-ROM Prosthesis. Total hip implant failed after six months in vivo. Patient (male, 60 yrs in age) indicated symptoms of pain and device failure to his surgeon.

E N D
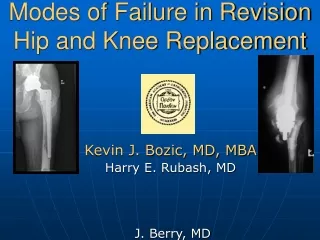
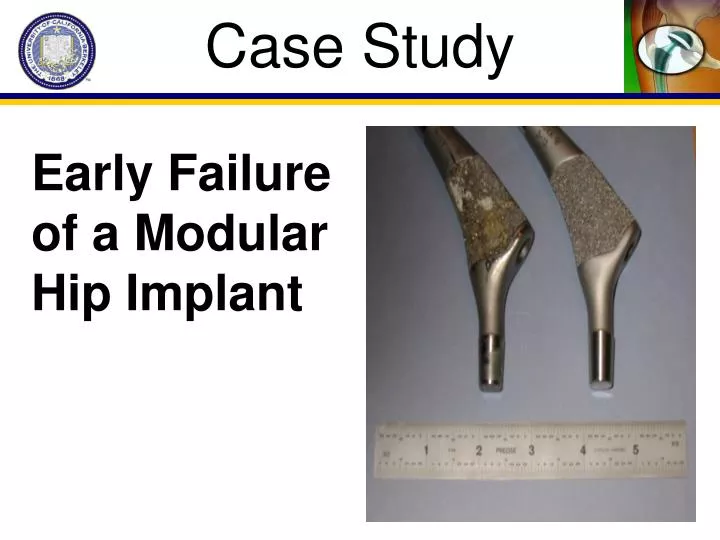
Case Study Early Failure of a Modular Hip Implant
Summary of Failed S-ROM Prosthesis • Total hip implant failed after six months in vivo. • Patient (male, 60 yrs in age) indicated symptoms of pain and device failure to his surgeon. • Howmedica SROM with a 42 mm neck and a 28 mm head. A +12mm skirt was used in this device. The acetabular liner was a Howmedica polyethylene shell with a 20mm inside diameter and a 54mm outside diameter. • Upon retrieval, the surgeon noted a large amount of white fluid with black particulate in the hip joint. The surgeon noted that there was a substantial amount of corrosion at the Morse taper and that it had a burnished appearance.
Typical Failure Analysis • How is a failure analysis conducted? • Collect medical report. Histological analysis and x-rays. What materials and design used? • Visual observation of device. Note any irregularities. • Optical micrographs to capture all damage on device. Comparison to pristine device. • Chemical and mechanical analysis. • Scanning electron microscopy to look for micromechanisms of fracture.
Failure Analysis • Once the failed device was explanted it was documented with both optical and electron microscopy. • Clear evidence of burnishing, pitting, and crevice corrosion were present on the device. Especially prevalent in the region of the Morse taper. • Scanning electron microscopy of the retrieval revealed intergranular attack and pitting associated with crevice corrosion and burnishing or scratching indicative of micromotion or fretting.
Burnishing/ Fretting
Burnishing/Fretting Corrosion
SEM Analysis of Taper Intergranular attack
Scientific Assessment • Fretting • Initial tolerance mismatch • stresses associated with the long neck (+12 mm neck) • Devices exceeding designed tolerances can lead to poor mechanical stability and may disrupt the interference fit required for long term structural integrity at the taper (Jacobs et al. 1998) • Brown et al. (1995) has shown a correlation between neck extension and fretting corrosion. Longer necks contribute to higher bending moments and enhance relative motion between the head and stem. It is postulated that fretting leads to a continuous passive film breakdown and repassivaton leading to oxygen consumption within the crevice. • The fractography of the failed device exhibits burnishing (associated with fretting), an etched microstructure associated with low pH, and pitting associated with crevice corrosion.
Possible solutions • Possible alternatives to prevent corrosion in Co-Cr heads coupled with Ti stems: (I) use hardened Ti head on Ti stem (II) use a cobalt-on-cobalt system (III) use a ceramic head on Ti or Co stem (IV) eliminate fluid from tapered interface (V) use self-locking mechanism to prevent fretting
Important Elements of the Case • Corrosion occurs in all metal implants(Jacobs et al, JBJS, 1998). • Corrosion is more prevalent in modular devices: corrosion observed in >30% of mixed alloy head/stem combinations vs. <6% all Cobalt alloy devices(Collier et al., Clin Orthop, 1995). • Biomechanical stresses are developed at the taper junction. Serves as a source of crevice corrosion (Gilbert et al., JBMR, 1993).
Taper Junction • Source of relative motion--fretting • Bending in the cone • Bending of the long neck extension (skirt) with proximal-distal slipping • Bore angle too large • Bore angle too small
Crevice corrosion • Micromotion between components results in fretting corrosion that can lead to initiation of crevice corrosion. • Metallic implants rely on passive oxide film for protection from corrosion. • Repetitive motion leads to continuous breakdown and repassivation. • Repeated breakdown consumes oxygen in crevice and results in drop in pH--crevice corrosion.
Crevice Corrosion OH- O2 OH- O2 O2 OH- OH- • Found in crevices or deep, narrow flaws (mismatch of components at interface • Can arise from localized oxygen depletion and metal ion concentration gradients
Mechanically Assisted Crevice Corrosion • In the head-neck taper, tolerances are such that narrow crevices exist with fluid present • At onset of loading, interfacial shear stresses are sufficient to fracture oxide film • Unpassivated metal is exposed to initially oxygen rich fluid. Oxidation occurs--depleting oxygen in crevice fluid--increases free metal ions--which attract Cl ions-->metal chlorides • Metal chlorides react with water to form metal hydroxide and HCl--lowers pH • Cr2O3 is unstable below pH of 3-- results in active attack of CoCr alloy--etched appearance (intergranular attack)
Multifactorial problem--depends on geometry, metallurgy, stresses, solution chemistry Driven by two primary factors: thermodynamic driving forces (Oxidation/Reduction) and kinetic barriers An electro-chemical attack resulting in material degradation Exacerbated by mechanical and biological attack Compromises Material Properties Mechanical Integrity Biocompatibility Aesthetics Corrosion Basics
Corrosion Basics • Occurs mostly in ionic, aqueous environments • Primarily a concern for metals • Oxidation – Reduction Reaction: • Loss of metal • Become ions in solutions • Combine with other species to form compound (oxides, hydroxides) • M → Mn+ + ne- • nH+ + ne- → nH
Uniform Attack • General corrosion that is evenly distributed over entire corrosion region • Rusting of iron, tarnishing of silverware • Most readily detectable (visual) and preventable (alloying)
Galvanic Corrosion • Two different metals/alloys that are in close proximity in an electrolytic environment • Distinct tendencies toward oxidation • Common in orthopaedics – Modular implants • Titanium femoral stems coupled with CoCr heads M+ N+ M+ e- N+ nM = nM+ +ne- nN+ + ne- = N M+ N+ M N M+ N+ N+ Metal 1 Metal 2
Crevice Corrosion OH- O2 OH- O2 O2 OH- OH- • Found in crevices or deep, narrow flaws (mismatch of components at interface • Can arise from localized oxygen depletion and metal ion concentration gradients
Pitting Corrosion • Subset of Crevice Corrosion • Formation of pits: local thickness reduction • Difficult to detect O2 O2 O2 OH- OH- OH- Cl- Cl- H+ H+ M+ M+ M+ M+ Cl- Cl- H+ M+ H+ http://www.materialsengineer.com/dup%20image/corrosion%2005b.jpg
Intergranular Corrosion • Preferential attack along grain boundaries • Results from localized differences in chemistry • Common in SS, nickel some Al alloys Sensitive Regions precipitates http://www.corrosionresolutions.com/example_diagnostic_photographs.htm
Fretting • Wear process due to relative motions in highly loaded devices exaggerated by corrosive environment • asperities of contacting surface • Device micromotions Load Relative Motion
Environmental Factors • Ion concentraion • Fluid velocities • Human Body – Conducive to Corrosion • Acidic – High ionic (H+)concentration • Aqueous (Blood, Synovium) – fluid flow • 37 C – Elevated Temperature
Importance to Implants • Mechanical Properties • Enhanced risk of crack propagation and fatigue fracture • Biocompatibility – Presence of metal ions triggers enhanced foreign body response • Osteolysis, implant loosening • Blood clotting (thrombosis)
Importance to Implants • Long term stability of metal implants critical for patient health & survival: • Stents • Arthoplasty • Fracture Fixation • Pacemakers