Download
1 / 81
810 likes | 929 Views
Dúvidas denucci@gdenucci.com Site www. gdenucci.com Arquivo Arritmias e insuficiência cardíaca congestiva. Electrocardiograms. Isoelectric point. R. T. P. S. Q. Normal ECG. Ventricular premature beat. Ventricular tachycardia. Ventricular fibrillation.

E N D
Dúvidas denucci@gdenucci.com Site www.gdenucci.com Arquivo Arritmias e insuficiência cardíaca congestiva
Electrocardiograms Isoelectric point R T P S Q Normal ECG Ventricular premature beat Ventricular tachycardia Ventricular fibrillation Int. Pharmacology – Chapter 18
Normal electrocardiogram Textbook of Medical Physiology – Guyton & Hall – Fig11.1
Above, Monophase action potential from a ventricular muscle fiber during normal cardiac function, showing rapid depolarization and then repolarization occurring slowly during the plateau stage but rapidly toward the end. Below, Electrocardiogram recorded simultaneously Textbook of Medical Physiology – Guyton & Hall – Fig11.3
Normal electrocardiograms recorded from the three standard electrocardiographic leads Textbook of Medical Physiology – Guyton & Hall – Fig11.7
Normal electrocardiograms recorded from the six standard chest leads Textbook of Medical Physiology – Guyton & Hall – Fig11.9
Normal electrocardigrams recorded from the three augmented unipolar limb leads Textbook of Medical Physiology – Guyton & Hall – Fig11.10
A Normal 12-leadECG recording. The recording were obtained synchronously, tree leads at a time ( I, II and III simultaneously) A 1-mV, 200-msec calibration pulse is visible in the three top recordings Medical Physiology – Boron &Boupaep – fig.20-10
A Normal 12-leadECG recording. The recording were obtained synchronously, tree leads at a time ( aVR, aVL, and aVF simultaneously) A 1-mV, 200-msec calibration pulse is visible in the three top recordings Medical Physiology – Boron &Boupaep – fig.20-10
A Normal 12-leadECG recording. The recording were obtained synchronously, tree leads at a time (V1, V2, and V3 simultaneously) A 1-mV, 200-msec calibration pulse is visible in the three top recordings Medical Physiology – Boron &Boupaep – fig.20-10
A Normal 12-leadECG recording. The recording were obtained synchronously, tree leads at a time (V4, V5, V6 simultaneously) A 1-mV, 200-msec calibration pulse is visible in the three top recordings Medical Physiology – Boron &Boupaep – fig.20-10
Pathological ECGs A- Normal Sinus Rhythm Medical Physiology – Boron &Boupaep – fig.20-13
Pathological ECGs B- First-Degree Block Medical Physiology – Boron &Boupaep – fig.20-13
Pathological ECGs C- Second-Degree Block:Möbitz Type I Medical Physiology – Boron &Boupaep – fig.20-13
Pathological ECGs C- Second-Degree Block:Möbitz Type II Medical Physiology – Boron &Boupaep – fig.20-13
Pathological ECGs E- Bundle Branch Blocks Medical Physiology – Boron &Boupaep – fig.20-13
Pathological ECGs F- Third-Degree Block Medical Physiology – Boron &Boupaep – fig.20-13
Pathological ECGs G- Delta Wave (Wolf-Parkinson-White Syndrome) Medical Physiology – Boron &Boupaep – fig.20-13
Pathological ECGs H- Atrial Fibrillation Medical Physiology – Boron &Boupaep – fig.20-13
Pathological ECGs Ventricular Fibrilation Ventricular tachycardia Ventricular Fibrillation Sinus rhythm Medical Physiology – Boron &Boupaep – fig.20-13
Purkinje fibers Re-entry of wave into tissue recently excited Conduction block ventricle Retrograde conduction Slow conduction Main mechanisms of arrhythmogenesis Int. Pharmacology – Chapter 18
Vaughan Williams classification of antiarrhythmic drugs Electrophysiologic actions Class Type of drug Examples I a Na+ channel Blocks conduction Quinidine blocker increases ERP Disopyramide I b Na+ channel Blocks conduction Lidocaine blocker decreases ERP Mexiletine I c Na+ channel Blocks conduction Flecainide blocker no effect on ERP, Encainide Int. Pharmacology – Chapter 18
Vaughan Williams classification of antiarrhythmic drugs Electrophysiologic actions Class Type of drug Examples II β Adrenoceptor Decreases sinus Propranolol antagonist node automaticity Sotalol Sympatholytic activity III A drug that No effects on Bretylium prolongs the conduction, delays Amiodarone action potential repolarization Sotalol duration IV Ca2+ antagonist Slow conduction Verapamil velocity in the Diltizem atrioventricular node Int. Pharmacology – Chapter 18
Quinidina • Primeiro antiarrítmico utilizado (1918) • Classificando como Ia • Bloqueia canais de Na e K • Aumenta intervalo QT (bloqueio dos canais de K) • Aumenta concentrações de digoxina • Aumenta morte súbita no tratamento de arritmias • Pode causar taquicardia paroxística • Uso terapêutico na síndrome do QT curto
! Adverse effects of quinidine ● Nausea ● Fever ● Syncope ● Blood dyscrasia ● Torsades de pointes Int. Pharmacology – Chapter 18
Vaughan Williams classification of antiarrhythmic drugs Electrophysiologic actions Class Type of drug Examples I a Na+ channel Blocks conduction Quinidine blocker increases ERP Disopyramide I b Na+ channel Blocks conduction Lidocaine blocker decreases ERP Mexiletine I c Na+ channel Blocks conduction Flecainide blocker no effect on ERP, Encainide Int. Pharmacology – Chapter 18
Procainamida • Propriedades similares a quinidina • Mais rapidamente absorvida por via oral • Profilaxia de taquicardia ventricular • Não há evidência de redução de morte súbita na FV ou no IAM
Vaughan Williams classification of antiarrhythmic drugs Electrophysiologic actions Class Type of drug Examples I a Na+ channel Blocks conduction Quinidine blocker increases ERP Disopyramide I b Na+ channel Blocks conduction Lidocaine blocker decreases ERP Mexiletine I c Na+ channel Blocks conduction Flecainide blocker no effect on ERP, Encainide Int. Pharmacology – Chapter 18
Lidocaína • Antiarrítmico Ib • Administrado por via intravenosa (alto metabolismo hepático) • Não melhora sobrevida no IAM • Utilizada em taquiarritmias ventriculares • Utilizada como anestésico e analgésico (local ou sistêmico)
Vaughan Williams classification of antiarrhythmic drugs Electrophysiologic actions Class Type of drug Examples I a Na+ channel Blocks conduction Quinidine blocker increases ERP Disopyramide I b Na+ channel Blocks conduction Lidocaine blocker decreases ERP Mexiletine I c Na+ channel Blocks conduction Flecainide blocker no effect on ERP, Encainide Int. Pharmacology – Chapter 18
Flecainide • Clássico Ic • Alargamento do QRS • Utilizado somente para tratamento de TSV • Aumenta o risco de morte súbita no IAM
Survival of patients in the Cardiac Arrhythmia Suppression Trial 100 95 90 85 0 Survival (%) P = 0.0006 0 50 100 150 200 250 300 350 400 450 500 Days after randomization to treatment group Placebo (number of patients = 725) Encainide or flecainide (number of patients = 730) Study terminated on ethical grounds Int. Pharmacology – Chapter 18
Vaughan Williams classification of antiarrhythmic drugs Electrophysiologic actions Class Type of drug Examples II β Adrenoceptor Decreases sinus Propranolol antagonist node automaticity Sotalol Sympatholytic activity III A drug that No effects on Bretylium prolongs the conduction, delays Amiodarone action potential repolarization Sotalol duration IV Ca2+ antagonist Slow conduction Verapamil velocity in the Diltizem atrioventricular node Int. Pharmacology – Chapter 18
Molecular mechanism of action of β1adrenoceptor antagonists catecholamine β1 adrenoceptor Adenylyl cyclase Cell membrane αs β γ cAMP ATP Kinase (active) Kinase (inactive) phosphorylation Contraction of heart muscle Int. Pharmacology – Chapter 18
Sotalol • Bloqueia canais de K • Utilizado na profilaxia de fibrilação atrial pós-operativa • d-Sotalol não apresenta atividade beta bloqueadora
Vaughan Williams classification of antiarrhythmic drugs Electrophysiologic actions Class Type of drug Examples II β Adrenoceptor Decreases sinus Propranolol antagonist node automaticity Sotalol Sympatholytic activity III A drug that No effects on Bretylium prolongs the conduction, delays Amiodarone action potential repolarization Sotalol duration IV Ca2+ antagonist Slow conduction Verapamil velocity in the Diltizem atrioventricular node Int. Pharmacology – Chapter 18
Amiodarona • Causa aumento de intervalo QT • Classe III, entretanto bloqueia canais de Na e CA, assim como alfa adrenoceptores • Diminui expressão de receptores beta1 • Eficaz no tratamento de TSV e TV
! Adverse effects of amiodarone ● Thyroid abnormalities ● Corneal deposits ● pulmonary disorders ● Skin pigmentation Int. Pharmacology – Chapter 18
Vaughan Williams classification of antiarrhythmic drugs Electrophysiologic actions Class Type of drug Examples II β Adrenoceptor Decreases sinus Propranolol antagonist node automaticity Sotalol Sympatholytic activity III A drug that No effects on Bretylium prolongs the conduction, delays Amiodarone action potential repolarization Sotalol duration IV Ca2+ antagonist Slow conduction Verapamil velocity in the Diltizem atrioventricular node Int. Pharmacology – Chapter 18
Verapamil • Classe IV • Diminui a frequência no SA • Diminui a condução do nódulo AV • Efeito inotrópico negativo • Vasodilatação coronária • Utilizado no tratamento de TSV
! ! Adverse effects of verapamil ● Bradycardia ● Nausea and vomiting ● Constipation Adverse effects of adenosine ● acceleration of tachycardia in Wolff-Parkinson-White syndrome ● Atrial fibrillation in Wolff-Parkinson-White syndrome ● Bronchospasm and hypotension Int. Pharmacology – Chapter 18
! Adverse effects of Ca2+ antagonists Nifedipine Verapamil / diltiazem ● Dizziness ● Bradycardia ● Flushing ● Hypotension ● Hypotension ● Congestive heart failure ● Skin rash ● Heart block ● Peripheral edema ● Skin rash ● Tachycardia ● Constipation Int. Pharmacology – Chapter 18
Common diseases that contribute to the development of congestive heart failure ● Cardiomyopathy ● Myocardial ischemia and infarction ● Hypertension ● Cardiac valve disease ● Congenital heart disease ● Coronary artery disease Clinical features of congestive heart failure ● Reduced force of cardiac contraction ● Reduced cardiac output ● Reduced tissue perfusion ● Increased peripheral vascular restance ● Edema Int. Pharmacology – Chapter 18
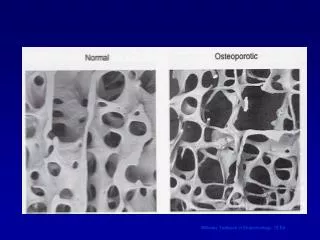
Types of cardiomyopathies involving both the right and the left ventricle Dilated (congestive) heart Normal heart Hypertrophic heart Int. Pharmacology – Chapter 18
Mechanism of action of digitalis glycosides Int. Pharmacology – Chapter 18
Heart Failure: Treatment Bronchus Pulmonary circulation Alveolus Antihistaminics Defoaming agents (alcohol) Cerebrum Sedation, reserpine Diuretics Oxygen Medulla Spinal anesthesia Spinal cord Nitrates Left Heart Ganglionic blockers Right Heart Digitalis Tourniquets Thrombolytics Venesection Digitalis (a glycoside) ACE inhibitors Adrenolytics sympatholytics Sugar
! Adverse effects of drugs used in the treatment of congestive heart failure ● Cardiac glycosides have a narrow therapeutic index and may precipitate arrhythmias ● Short-term treatment with phosphodiesterase inhibitors can cause thrombocytopenia and arrhythmias ● β1Agonists may precipitate tachyarrhythmias, and long-term use may worse myocardial function ● Diuretics produce serious electrolyte imbalances such as hypokalemia, which may produce ventricular arrhythmias ● Angiotensin-converting enzyme (ACE) inhibitors produce few adverse effects, andgenerally only hypotension ● Nitrovasodilators have few adverse effects Int. Pharmacology – Chapter 18
Hypertension Treatment: Angiotensin-Converting Enzyme Inhibitors ACE inhibitors Liver Adrenal Renin substrate (angiotensinogen) Angiotensin I Angiotensin II Medulla Angiotensin-converting enzyme (ACE) Cortex Renin Angiotensin promotes output of aldosterone Vasoconstru]iction Aldosterone promotes Na+ and H2O retention, K+ excretion, and arteriolar constriction Compression of extrarenal or intrarenal vessels promotes output renin by juxtaglomerular cells Captopril (an ACE inhibitor)