Download
1 / 1
10 likes | 226 Views
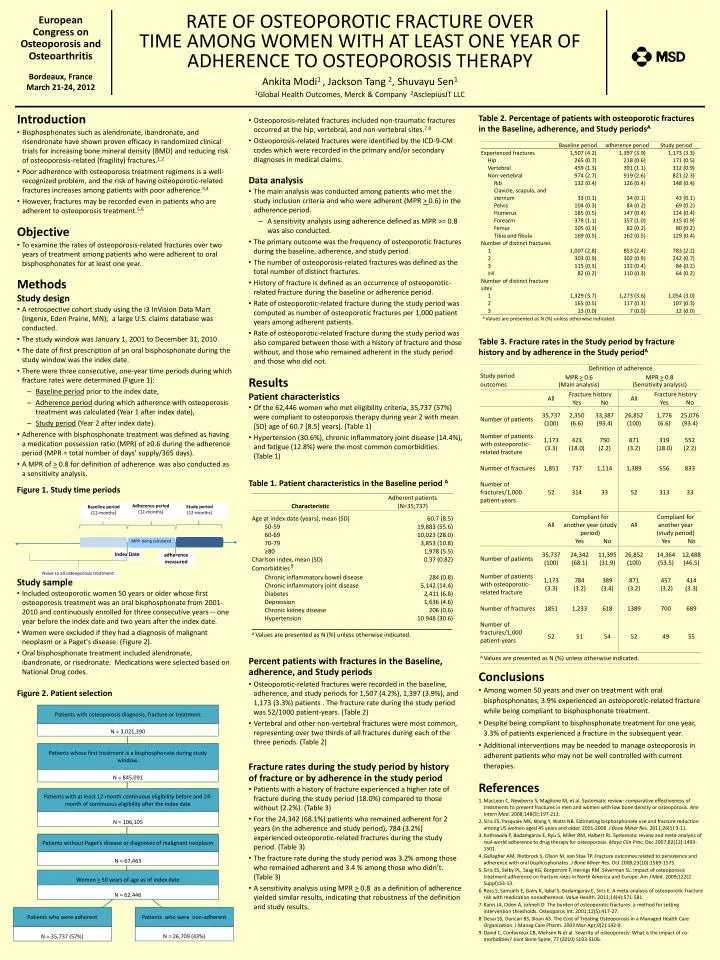
Patients with osteoporosis diagnosis, fracture or treatment. Adherence period (12-months). N = 3,021,390. Patients whose first treatment is a bisphosphonate during study window. N = 845,091.

E N D
Patients with osteoporosis diagnosis, fracture or treatment Adherence period (12-months) N = 3,021,390 Patients whose first treatment is a bisphosphonate during study window. N = 845,091 Patients with at least 12-month continuous eligibility before and 24-month of continuous eligibility after the index date N = 106,105 Study period (12-months) Patients without Paget's disease or diagnoses of malignant neoplasm N = 67,463 Baseline period (12-months) Women > 50 years of age as ofindex date N = 62,446 Patients who were non-adherent Patients who were adherent N = 26,709 (43%) N = 35,737 (57%) RATE OF OSTEOPOROTIC FRACTURE OVER TIME AMONG WOMEN WITH AT LEAST ONE YEAR OF ADHERENCE TO OSTEOPOROSIS THERAPY Ankita Modi1 , Jackson Tang 2, Shuvayu Sen1 1Global Health Outcomes, Merck & Company 2AsclepiusJT LLC European Congress on Osteoporosis and Osteoarthritis MPR being calculated adherence measured Index Date Naive to all osteoporosis treatment Bordeaux, France March 21-24, 2012 • Introduction • Bisphosphonates such as alendronate, ibandronate, and risendronate have shown proven efficacy in randomized clinical trials for increasing bone mineral density (BMD) and reducing risk of osteoporosis-related (fragility) fractures.1,2 • Poor adherence with osteoporosis treatment regimens is a well-recognized problem, and the risk of having osteoporotic-related fractures increases among patients with poor adherence.3,4 • However, fractures may be recorded even in patients who are adherent to osteoporosis treatment.5,6 Table 2. Percentage of patients with osteoporotic fractures in the Baseline, adherence, and Study periodsA • Osteoporosis-related fractures included non-traumatic fractures occurred at the hip, vertebral, and non-vertebral sites.7.8 • Osteoporosis-related fractures were identified by the ICD-9-CM codes which were recorded in the primary and/or secondary diagnoses in medical claims. • Data analysis • The main analysis was conducted among patients who met the study inclusion criteria and who were adherent (MPR > 0.6) in the adherence period. • A sensitivity analysis using adherence defined as MPR >= 0.8 was also conducted. • The primary outcome was the frequency of osteoporotic fractures during the baseline, adherence, and study period. • The number of osteoporosis-related fractures was defined as the total number of distinct fractures. • History of fracture is defined as an occurrence of osteoporotic-related fracture during the baseline or adherence period. • Rate of osteoporotic-related fracture during the study period was computed as number of osteoporotic fractures per 1,000 patient years among adherent patients. • Rate of osteoporotic-related fracture during the study period was also compared between those with a history of fracture and those without, and those who remained adherent in the study period and those who did not. • Objective • To examine the rates of osteoporosis-related fractures over two years of treatment among patients who were adherent to oral bisphosphonates for at least one year. • Methods • Study design • A retrospective cohort study using the i3 InVision Data Mart (Ingenix, Eden Prairie, MN); a large U.S. claims database was conducted. • The study window was January 1, 2001 to December 31, 2010. • The date of first prescription of an oral bisphosphonate during the study window was the index date. • There were three consecutive, one-year time periods during which fracture rates were determined (Figure 1): • Baseline period prior to the index date, • Adherence period during which adherence with osteoporosis treatment was calculated (Year 1 after index date), • Study period (Year 2 after index date). • Adherence with bisphosphonate treatment was defined as having a medication possession ratio (MPR) of ≥0.6 during the adherence period (MPR = total number of days’ supply/365 days). • A MPR of > 0.8 for definition of adherence was also conducted as a sensitivity analysis. Table 3. Fracture rates in the Study period by fracture history and by adherence in the Study periodA • Results • Patient characteristics • Of the 62,446 women who met eligibility criteria, 35,737 (57%) were compliant to osteoporosis therapy during year 2 with mean [SD] age of 60.7 [8.5] years). (Table 1) • Hypertension (30.6%), chronic inflammatory joint disease (14.4%), and fatigue (12.8%) were the most common comorbidities. (Table 1) Table 1. Patient characteristics in the Baseline period A Figure 1. Study time periods • Study sample • Included osteoporotic women 50 years or older whose first osteoporosis treatment was an oral bisphosphonate from 2001-2010 and continuously enrolled for three consecutive years -- one year before the index date and two years after the index date. • Women were excluded if they had a diagnosis of malignant neoplasm or a Paget's disease. (Figure 2). • Oral bisphosphonate treatment included alendronate, ibandronate, or risedronate. Medications were selected based on National Drug codes. • Percent patients with fractures in the Baseline, • adherence, and Study periods • Osteoporotic-related fractures were recorded in the baseline, adherence, and study periods for 1,507 (4.2%), 1,397 (3.9%), and 1,173 (3.3%) patients . The fracture rate during the study period was 52/1000 patient-years. (Table 2) • Vertebral and other non-vertebral fractures were most common, representing over two thirds of all fractures during each of the three periods. (Table 2) • Conclusions • Among women 50 years and over on treatment with oral bisphosphonates, 3.9% experienced an osteoporotic-related fracture while being compliant to bisphosphonate treatment. • Despite being compliant to bisphosphonate treatment for one year, 3.3% of patients experienced a fracture in the subsequent year. • Additional interventions may be needed to manage osteoporosis in adherent patients who may not be well controlled with current therapies. Figure 2. Patient selection • Fracture rates during the study period by history • of fracture or by adherence in the study period • Patients with a history of fracture experienced a higher rate of fracture during the study period (18.0%) compared to those without (2.2%). (Table 3) • For the 24,342 (68.1%) patients who remained adherent for 2 years (in the adherence and study period), 784 (3.2%) experienced osteoporotic-related fractures during the study period. (Table 3) • The fracture rate during the study period was 3.2% among those who remained adherent and 3.4 % among those who didn’t. (Table 3) • A sensitivity analysis using MPR > 0.8 as a definition of adherence yielded similar results, indicating that robustness of the definition and study results. • References • MacLean C, Newberry S, Maglione M, et al. Systematic review: comparative effectiveness of treatments to prevent fractures in men and women with low bone density or osteoporosis. Ann Intern Med. 2008;148(3):197-213. • Siris ES, Pasquale MK, Wang Y, Watts NB. Estimating bisphosphonate use and fracture reduction among US women aged 45 years and older, 2001-2008. J Bone Miner Res. 2011;26(1):3-11. • Kothawala P, Badamgarav E, Ryu S, Miller RM, Halbert RJ. Systematic review and meta-analysis of real-world adherence to drug therapy for osteoporosis. Mayo Clin Proc. Dec 2007;82(12):1493-1501. • Gallagher AM, Rietbrock S, Olson M, van Staa TP. Fracture outcomes related to persistence and adherence with oral bisphosphonates. J Bone Miner Res. Oct 2008;23(10):1569-1575. • Siris ES, Selby PL, Saag KG, Borgstrom F, Herings RM, Silverman SL. Impact of osteoporosis treatment adherence on fracture rates in North America and Europe. Am J Med. 2009;122(2 Suppl):S3-13. • Ross S, Samuels E, Gairy K, Iqbal S, Badamgarav E, Siris E. A meta-analysis of osteoporotic fracture risk with medication nonadherence. Value Health. 2011;14(4):571-581. • Kanis JA, Oden A, Johnell O. The burden of osteoporotic fractures: a method for setting intervention thresholds. Osteoporos Int. 2001;12(5):417-27. • Desai SS, Duncan BS, Sloan AS. The Cost of Treating Osteoporosis in a Managed Health Care Organization. J Manag Care Pharm. 2003 Mar-Apr;9(2):142-9. • David C, Confavreux CB, Mehsen N et al. Severity of osteoporosis: What is the impact of co-morbidities? Joint Bone Spine, 77 (2010) S103-S106.






