Download
1 / 83
860 likes | 1.16k Views
CHIKUNGUNYA FEVER. Dr. R.V.S.N. Sarma M.D., M.Sc. (Canada), FIMSA Consultant Physician and Cardiometabolic Specialist. www.drsarma.in. What is this tongue twister ?. It is CHIKUNGUNYA To be pronounced as [chick’-en-GUN-yah] It is not written as CHICKEN GUINEA

E N D
CHIKUNGUNYA FEVER Dr. R.V.S.N. Sarma M.D., M.Sc. (Canada), FIMSA Consultant Physician and Cardiometabolic Specialist www.drsarma.in
What is this tongue twister ? • It is CHIKUNGUNYA • To be pronounced as [chick’-en-GUN-yah] • It is not written as CHICKEN GUINEA • Nothing to do with chicken or mutton eating • Derived from the Makonde verb - Kun gunyala • In Swahili it means ‘to become contorted’ or • More specifically as ‘that which bends up’ • Refers to the stooped posture of the patient
Synonyms • CHIKV Fever • Buggy Creek virus infection • Knuckle fever • Me Tri virus infection • Semliki Forest virus infection
Blessed are we !! • This is not a Dengue epidemic ! • This is not the SARS which stole all the show !! • This is not Bird-Flu hitting Indian economy !!! • This is not the Plague epidemic which threatened to sweep our country !!!! • It is not the H1N1 that occupied the media time !!! • Above all - it is not like HIV or Hepatitis B !!!!! • This is a self limiting, non fatal viral illness – Thanks to the Almighty
Should we be panicky ? • A common viral fever • Self limiting – non fatal illness • Fever, myalgia, arthralgia, lasting 2 - 7 days • Should we give big name for it and be panicky ? • Should we create such media hype and chaos ? • Above all, should we politicize to this extent?
CLINICAL EPIDEMIOLOGY www.drsarma.in
www.drsarma.in A Disease of Africa and Asia
www.drsarma.in Asian Distribution
www.drsarma.in Epidemiological Triangle The Environment The Vector Interaction The Host The Virus
www.drsarma.in History (Its story) • A viral infection transmitted to humans • By the bite of an infected mosquito • It has become endemic in south and central India • First outbreak in 1952 on the Makonde Plateau • Border between Tanganyika and Mozambique • First published report is from Africa in 1955 by • Marion Robinson and W.H.R. Lumsden • Recent large epidemic occurred in Malaysia in 1999
The CHIK Virus www.drsarma.in
www.drsarma.in What is this virus ? • Causative agent is an RNA – VIRUS • Class – Arbor Virus (Arthropod Borne) • Family – Togaviridae • Genus – Alpha Virus • Species – Chikungunya Virus • Similar to Semliki Forest Viruses (SFV) in Africa and Asia.
www.drsarma.in Chikungunya Virus - EM
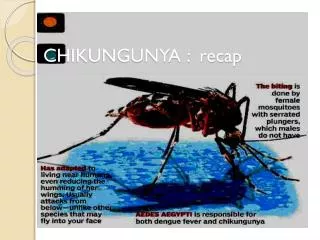
www.drsarma.in Transmission • Reservoir – Non-human primates in Africa • No animal reservoir is found in India • Maintained in nature by man – mosquito – man • Vector – Aedes aegypti, Ae. albapticus mosquito • Same vector as for Dengue and Yellow fevers • Vehicle of transmission – None (only mosquito) • No known mode - other than mosquito bite • Incubation Period – 2 days to 12 days
The Vector www.drsarma.in
www.drsarma.in The Vector • Aedes aegypti mosquito, flight range < 100 meters • Aggressive daytime biter –bites ankles • Once infected – it has the virus until death (30 day) • It is a man made mosquito – prefers its owner • Breeds in man made household containers • Indoor, peri domestic, fresh water mosquito • Metallic, plastic, rubber, cement and earthen containers - open, left or unused - filled with water • Air coolers, ACs, Old oil drums, Over head tanks
www.drsarma.in Aedes aegypti
www.drsarma.in Aedes albaptycus Tiger Mosquito
www.drsarma.in Madam Aedes - at her Lunch
www.drsarma.in Water tap – A disease trap
www.drsarma.in Open Overhead Tanks
Domestic Water Collections www.drsarma.in
Why only Aedes Mosquito ? • Scanning Electron Micro-graph of the mid gut cells of the mosquito • Location of the Chik Virus binding proteins. • Not transmitted to the progeny of the mosquito www.drsarma.in
The Recent Epidemics www.drsarma.in
www.drsarma.in Notable Outbreaks • 1963 to 1965 - An epidemic was reported in Calcutta – • 4.37% of the people were found to be sero positive • 1973 – An epidemic 37.53% in Barsi - Sholapur • 2006 – Present epidemic after 33 years is the largest • 9,06, 360 or more cases in Andhra Pradesh • 5,43, 286 cases from Karnataka; 66,109 from B’lore • Maharashtra 2,02,114 cases; Gujarat 2,500 cases • Tamil Nadu 49,567 cases; Orissa 4,904 cases, • Madhya Pradesh 43,784 and Pune 138 cases
www.drsarma.in Distribution in India • The disease is common with periodic epidemics • Sporadic outbreaks described in Madras and Vellore • Cases were reported in Chennai, Pondicherry, Vellore • Vizag in 1964; Rajahmundri, Kakinada, Nagpur in 1965 • The last epidemic in India was in 1973 • From Yavat village (Pune) in 2000 • 2.9% in the Andaman & Nicobar Islands seropositive • Infected mosquitoes seen in Pune, Maharastra State
www.drsarma.in Most Recent Epidemics • Epidemic of CHIKV occurred in Malaysia – 1999 • French island of Réunion in the Indian Ocean- ‘05 • Epidemic was recorded in Mauritius – 2005 • Madagascar, Mayotte and Seychelles – 2005 • Hong Kong and Malaysia early 2006 • Present Indian epidemic is the largest -from Dec ’05 • Maximum # of cases from Andhra Pradesh so far
www.drsarma.in The Indian Epidemic • Present epidemic has started in Nov 2005 • Andhra Pradesh, Karnataka, Maharashtra, Madhya Pradesh, Orissa, Gujarat, Tamilnadu, Rajasthan, Kerala are under its onslaught • This is spreading far and wide at a rapid rate • Not much spread to the northern states like Delhi, Haryana, Punjab as yet. • Not much cry from U.P. and Bihar
www.drsarma.in Attack Rates • In urban localities it is more – why ? • Usual age group is above 15 years • Less common in children and infants • Family clustering of cases usual • Attack rates vary from 3 to 40% of population • Average attack rate is 10% • Herd immunity restricts further spread
www.drsarma.in Why is this sudden epidemic ? Analysis of the recent Indian epidemic has suggested that the increased severity of the disease is due to a change in the genetic sequence, altering the virus’ coat protein, which potentially allows it to multiply more easily in mosquito cells*. *http//medicine.plosjournals.org
www.drsarma.in Why is this quasi-pandemic ? • Several distinct variants of the virus • A change at position 226 of the E1 coat protein • This A226V mutation caused the virus to more easily invade and multiply in the mosquitoes • Three protein changes in non-structural proteins nsP1 (T301I), nsP2 (Y642N), and nsP3 (E460 deletion) This mutant virus - from a neonatal encephalopathy case
Clinical Features www.drsarma.in
www.drsarma.in Symptoms • Sudden onset of fever, chills • Headache, nausea, vomiting, abdominal pain • Joint pain with or usually without swelling • Low back pain and rash • Very similar to those of Dengue but • Unlike in Dengue, no hemorrhagic or shock syndrome
www.drsarma.in Clinical Features • Incubation period is 2-12 d; usually 3-7 days • Viremia last for 5 days (infective period) • Silent CHIKV – inapparent infections in children • Flu-like symptoms, Severe headache and chills • High grade fever (40°C or 104°F), • Arthralgia or arthritis – lasting several weeks • Conjunctival suffusion and mild photophobia • Nausea, vomiting, abd. pain, severe weakness
www.drsarma.in The Arthralgia • The small joints of the lower and upper limbs • Migratory poly arthralgia – not much effusions • Larger joints may also be affected (knee, ankle) • Pain worse in the morning – less by evening • Joints may be swollen & painful to the touch • Some patients have incapacitating joint pains • Arthritis may last for weeks or months.
www.drsarma.in Kun gunyala The Contorted Posture
www.drsarma.in Acute CHIKV Fever
www.drsarma.in Skin Rash in Dengue
www.drsarma.in Skin Rash in CHIKV
www.drsarma.in Petechiae on feet
www.drsarma.in The Burden of CHIKV
Rare Clinical Features • A petechial or maculo papular rash usually involving the limbs may occur. • Hemorrhage is rare • Nasal blotchy erythema, freckle-like pigmentation over centro-facial area, • Flagellate pigmentation on face and extremities • Lichenoid eruption and hyper pigmentation in exposed areas
www.drsarma.in Rare Clinical Features • Multiple aphthous-like ulcers over • scrotum, crural areas and axilla • Unilateral or bilateral lympoedema of the limbs • Lymphadenopathy not common • Multiple ecchymotic spots in children • Vesiculo-bullous lesions in infants and • Sub-ungual hemorrhages • Severe menigo-encephalitis – rare; may be fatal
www.drsarma.in Course of Illness • Fever typically lasts for 2 - 3 days and comes down • Fever may reoccur after 3 days – ‘saddle back’ fever • Some rare cases - fever lasts up to a couple of weeks • Patients do have prolonged fatigue for several weeks • High fever & crippling joint pain marked this epidemic • Joint pain, intense headache, insomnia and an extreme degree of prostration may last for 5 to 7 days • Life long immunity, once one suffers this infection
www.drsarma.in Who are at greater risk ? • Pregnant women • Elderly people • Newborns • Women in general • Diabetics • Immuno-compromised patients • Patients with severe chronic illnesses
www.drsarma.in CHIKV Morbidity • Chikungunya is a self-limiting illness • Causes of prolonged morbidity are • Severe dehydration • Electrolyte imbalance and • Loss of glycemic control • Recovery is the rule • In about 3 to 5% • Incidence of prolonged arthritis
www.drsarma.in Mortality • A few deaths have been reported – Reasons are • It was thought to be due mainly to • Inappropriate use of antibiotics and NSAIDs • Virus can cause thrombocytopenia • These drugs can cause gastric erosions - thus • Leading to fatal upper GI bleed • Use of steroids for the joint pains & inflammation • This is dangerous and completely unwarranted
Pregnancy and CHIKV www.drsarma.in