Download
1 / 34
350 likes | 469 Views
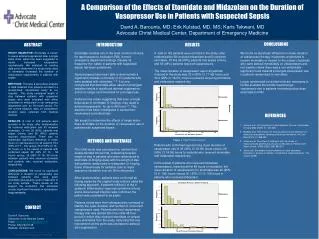
Directional Preference: Classification through Mechanical Assessment. Ron Donelson, MD, MS SelfCare First, LLC. Enter. Red Flags?. Classification through Mechanical Assessment and Diagnosis. Independent Management. Y. N. Y. Patient Specific Functional Reactivation.

E N D
Directional Preference: Classification throughMechanical Assessment Ron Donelson, MD, MS SelfCare First, LLC
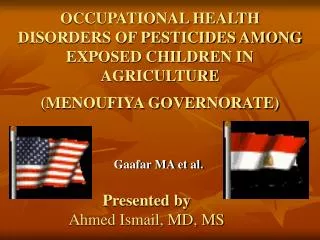
Enter Red Flags? Classification through Mechanical Assessment and Diagnosis Independent Management Y N Y Patient Specific Functional Reactivation Matched DirectionalExercises + Postures, Remains better N Re-Enter after Surgical/Interventional Y N YELLOW FLAGS Trunk Stabilization Adjunct Treatments PRN Active Rest, Activity Modification CBT, FRP, Manual Therapy Y N Directional Preference? N Maladaptive Motor Control Patterns? Prior Functional Level Fully Restored? Motor Control Restoration Y N Functional Optimization: Quota based exercise Instability? (Radiograph/Clinical) Surgical/Interventional Appropriate Candidate?
What I’ll cover: Context: Four challenges with our spine care dilemma. Where do we need to go? Directional preference: How it’s determined; Reliability and validity evidence; Why is it first in the algorithm? How does it impact the remaining algorithm and future research?
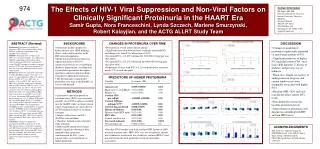
#1 Context: Our Dilemma “U.S. Spine Care System ina State of Continuing Decline”(BackLetter, Oct 2013) Mafi et al (2013) – National Ambulatory and Hospital Medical Care Survey: An acceleration of the development of chronic pain, work disability, more opioid prescriptions and narcotic addiction, use of injections and surgery, and guideline-discordant care. Mafi J, McCarthy E, Davis R, BE L. Worsening trends in the managementand treatment of back pain. JAMA Intern Med. 2013
A huge effort has been invested to improve RCT design and the Levels of Evidence research construct: • Systematic reviews typically conclude: “insufficient evidence”, “more research must be done” • Many treatments persist with little supportive evidence • Spine care costs keep increasing with no evidence of better outcomes WHY?
Every process is perfectly designedto get the results it gets. Paul Batalden Insanity: doing the same thing overand over again and expectingdifferent results. Albert Einstein.
#2 Context: A Fundamental Shortcoming Quebec Task Force Report: “There is so much variability in making a diagnosis that this initial step routinely introduces inaccuracies which are then further confounded with each succeeding step in care.” Spitzer, et al: Scientific approach to the assessment and management of activity-related spinal disorders (The Quebec Task Force). Spine, 1987. 12(7S): p. S16-21.
#2 Context: A Basic Clinical Shortcoming Quebec Task Force Report: The diagnosis “is the fundamental source of error….. Faced with uncertainty, physicians become inventive.” Spitzer, et al: Scientific approach to the assessment and management of activity-related spinal disorders (The Quebec Task Force). Spine, 1987. 12(7S): p. S16-21.
Clinical Guidelines? All Others! (Non-specific) Muscle Ligament SI Joint HNP Inflammation Internal Disc Subluxation Spondys Facet Red Flags Tumor Infection Fracture 85% “Black Box” Classification ConventionalClinical Examination “The fundamental source of error.” QTF Report HNP’s w/ Neuro Deficit “Diagnostic Triage”
#3 Context: A Glimpse at the Solution Intuitive Empirical Precision medicine • Intuitive: highly trained professionals solve med. problems through intuitive experimentation (“Experience-Based Medicine”) • Empirical: data amassed to show certain ways of treating patients on average (“Evidence-B medicine”) • Precision: diseases diagnosed precisely; standardized, predictably effective treatment that addresses the cause, not the symptom(Diagnosis-Based medicine”)
How precise are our diagnoses now? Red flags Convent’lClinical Exam HNP Our most precise anatomic diagnosis…. But how precise is it? 85% There is no standardized predictably-effective treatment. Non-Specific LBP
Our dilemma 85% - no diagnosis 10% - anatomic diagnosis, but it’s imprecise The best treatment for NS-symptom? RCTsGuidelinesLevels of Evidence Yet spine careis in decline! Need a paradigm shift!
#4 Two surveys of international LBP researchers: #1 LBP research priority: Identifying and validatingLBP subgroups Borkan, et al: A report from the second international forum for primary care research on low back pain: reexamining priorities. Spine. 1998 Costa, et al: Are we making progress? Spine, 2012
A-D-T-O Research Model for Validating Subgroups Outcome T-O Link Treatment D-T Link Diagnosis A-D Link Assessment RCTs that target NS-LBPare “doomed”. Subgroup RCTs: Which is the best treatment? To validate diagnostic subgroups that enhance individualized care…… Prospective subgrp cohorts: Does subgroup-specific treatment improve outcomes? Reliability studies:∙ test findings ∙ subgroup classification Kevin Spratt, AAOS 2003
Enter Red Flags? Classification through Mechanical Assessment and Diagnosis Independent Management Y N Y Patient Specific Functional Reactivation Matched DirectionalExercises + Postures, Remains better N Re-Enter after Surgical/Interventional Y N YELLOW FLAGS Trunk Stabilization Adjunct Treatments PRN Active Rest, Activity Modification CBT, FRP, Manual Therapy Y N Directional Preference? N Maladaptive Motor Control Patterns? Prior Functional Level Fully Restored? Motor Control Restoration Y N Functional Optimization: Quota based exercise Instability? (Radiograph/Clinical) Surgical/Interventional Appropriate Candidate?
Mechanical Diagnosis & Therapy (MDT): How would your car mechanic evaluate your car? A history A test-drive MDT - a dynamic mechanical test-drive:patients perform standardized end-range spine bendingand loading tests to see how the symptoms respond. Reproducible response patterns characterize & classify the underlying problem into mechanical subgroups: • most have subgroup-specific mechanical treatments • others have objective indications for other diagnostics
Extension 1 3 Flexion Reduce Centralize Abolish Directional Preference 2 Directional Vulnerability • Produce Increase Peripheralize Lateral Monitor Pain Response Relatedto Directional Loading Strategies Monitor Pain Response Related to Directional Loading Strategies MDT Key: perform movements repeatedly and to end-range. Single direction Insight: persistence / recurrences “Rapidly Reversible LBP”
How common is dir. pref.: a reducible derangement? Acute Chronic Prevalence of dir. pref. & centralization: Donelson (Spine 1990) 84-89 % Sufka (JOSPT, 1998) 60-83 % Werneke (Spine, 1999) 77 % Karas (Phys. Ther. 1997) 73 % Donelson (Spine 1991, ISSLS 1991) 58 % Delitto (Phys. Ther. 1993) 61 % Erhard (Phys. Ther. 1995) 55 % Kopp (CORR, 1986) 52 % Long (Spine, 1995) 43 % Donelson (Spine ,1997) 49 % Laslett (Spine Jrnl, 2005) 32 % Acute, Chronic Axial pain, Sciatica Degenerative disc Pseudo-claudication Spondys
Rapid recovery from current episode • Decreased recurrences (50-70% first yr) • not well-documented in the literature….yet • Where recurrence prevention is rewarded: payers’ claims data of 5,000 patients shows that re-utilization of services after MDT care: <10% • Immense cost savings What is the Treatment for a Dir. Pref? Matching Directional Exercises, Posture, Education
DP and centralization:clues that help make a diagnosis The underlying pain-generator is: 1. mechanical 2. reversible (mechanically, directional, & lasting) 3. likely something displaced (a “derangement”)
A derangement:a “patho-mechanical” diagnosis 2 types are identified by mechanical testing: • Reducible: a directional preference that centralizes the pain and restores full motion • Irreducible: no centralization or dir. pref.; every direction of testing increases or peripheralizes the pain
Patho-Anatomic vs. Patho-Mechanical Diagnosis? Patho-Anatomic Diagnosis: 1. disc herniation: MRI can’t differentiate betw a painful and non-painful finding. 2. even if it is: a. only 10% of LBP population; b. “imprecise”: doesn’t identify a standardized, effective treatment. Patho-Anatomic Diagnosis (reducible derangement):Reliable dx: a. 70-89% of population; b. the treatment is standardized and predictably-effective. A patho-mechanical diagnosis is far more precise thanknowing the anatomic identity of the pain source.
Anatomic AND mechanical diagnosis: The Use of Lumbar Extension in the Evaluation and Treatment of Patients with Acute Herniated Nucleus Pulposus: A Preliminary Report 67 pts. w/ sciatica + neural deficits Trial of Extension 34 (52%) reversible 33 (48%) irreversible 2-5 day: all 34 pain-free; no surgery 32 under-went surgery Extension: 3-4 sessions/day Same anatomic dx: 52% reducible, 48% irreducible der’ts If fully tested, 10-15% more had a dir. pref. Kopp, Alexander, et.al. CORR 202:211-8, 1986
Treating Dir. Pref. (N = 72) with 2 weeks of matching exercises Donelson R, Long A, Spratt K, Fung: Influence of DP on two clinical dichotomies: acute versus chronic pain and axial low back pain versus sciatica. PM&R, 2012
Reducible Derangement (DP/Cent’n) Literature 9: Formal MDT training:Kappa = 0.9, 0.823, 0.7 % agreement: 88-100% 2: Little MDT training: Kappa = .2 to .4 8 16 10 11
Reducible Derangement (DP/Cent’n) Literature Outcomes improve >7X if exercise dir. matches DP. 50% of disc surgeries avoided Acute, chronic, axial, sciatica: rapid recoveries in 2 weeks 8 16 10 11
Outcome Prediction(D-T Link) DP and Centralization are better than: • Gender • SLR • Neurological signs (QTF) • Pain duration • Pain location • Leg pain intensity • Overt pain behaviors • Non-organic physical signs • Fear of work activities • Perceived disability • Smoking
Reducible Derangement (DP/Cent’n) Literature 8 16 10 11
69 non-centralizers underwent TESIs. After TESIs, MDT exam repeated @ 1-year: 62% remained excellent w/o surgery 46% 22% Centralizers 16% 16% ?? 16% 46% 11% 73% Non-Centralizers van Helvoirt H, et. al. Transforaminal epidural steroid injections followed by Mechanical Diagnosis and Therapy to prevent surgery for lumbar disc herniation. Pain Medicine. 2014.
Why is Dir. Pref. Determination the First Stopin this Decision-Making Algorithm? • Strong evidence across the entire ADTO model • High prevalence of dir. pref. across all durations and all LBP presentations • Treatment is highly consistent with current guidelines: activity/movement, self-care educ’n, re-assurance • Safety: no known risk or reported complications • Meets Christensen’s ‘precise diagnosis” definition. • No question or controversy on Exer. Com.
Consequences of Starting WithDir. Pref. Determination • The DP subgroup, successfully treated and very large, leave a much smaller subset to move to next decision point. • Prior RCTs of NS-LBP: the DP subgroup was not excluded, so many with a dir. pref. are randomized and treated with a non-directional approach. • Future research: should follow the ADTO model and existing subgroup evidence. First: identify/exclude those with a dir. pref.
If operating on the wrong leg is considered a “medical error”, what do we call operating on (injecting) someone who doesn’t need it? John Wennberg, MD Dartmouth Atlas