Download
1 / 21
250 likes | 400 Views
Minimal Ovarian Stimulation. Jung-Hyun Cho, M.D. (Miz Medi Hospital). LH. FSH. Recruitment Selection Dominance Ovulation. FSH. LH. hCG. FSH. GnRH-a. Ultrashort. Short. Long. Disadvantages of COH. High costs of ovulatory drugs GnRH-agonist, r-FSH, r-hCG

E N D
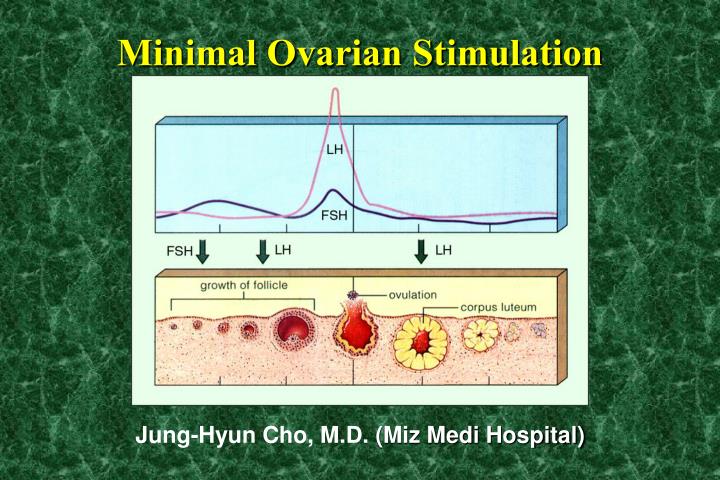
Minimal Ovarian Stimulation Jung-Hyun Cho, M.D. (Miz Medi Hospital)
LH FSH Recruitment Selection Dominance Ovulation
FSH LH hCG FSH GnRH-a Ultrashort Short Long
Disadvantages of COH • High costs of ovulatory drugs GnRH-agonist, r-FSH, r-hCG • Physical discomforts Daily injection of gonadotropins, Blood sampling • Time loss Daily visiting clinic, Frequent sonography • Risk of OHSS 5 ~ 10% of COH • Long term unkown risk of ovarian cancer
Concept of minimal ovarian stimulation • Less complex, Shorter stimulation regimens, Less expensive • Less patient discomfort, Less monitoring, Less programmable • Less chances of complications, Long term risks • Fewer oocytes for fertilization in vitro • Fewer spare embryos for cryopreservation
Applications of minimal ovarian stimulation • Natural cycle IVF-ET Kim KR (2000) • Oral contraceptives + Clomiphene 100mg x 8 days Branigan and Ester (2000) • GnRH antagonist + hMG Frydman R et al. (1999)
Natural cycle in IVF with GnRH antagonist Menstrual cycle E2 100 ~ 150 pg/ml Ø 12 ~ 14 mm M1 8 9 10 11 12 13 14 15 hMG hMG OPU ET Cetrorelix hCG Preg rate : 32.0% /ET Hum Reprod 14(3):683,1999 Frydman R et. al
IVM COH
Hypothetic scheme of immature oocyte IVF program In vitro maturation Immature oocyte retrieval Fertilization by ICSI Ovary : Immature oocytes Embryo development Uterus : Midproliferative endometrium E2 Biochemical assisted hatching Poliferative endometrium hCG Progesterone Embryo transfer Secretary endometrium Implantation
Oocyte pick up (OPU) Immature OPU COH - OPU Follicle size 5 - 10 mm 15 - 25 mm Needle diameter outer 17 G single 17 G inner 20 G Flushing media PBS PBS heparin 40 IU/ml Pressure 300 mmHg 100 mmHg Follicle curetting vigorous only suction Op. duration Long Short Anesthesia more deeper only sedation
Fertilization by ICSI Insemination-fertilization oocyte Zona hardening oocyte ICSI
Biochemical Assisted Hatching (BAH) by protease in conventional IVF(1994. 7. ~ 1996. 12.) - 1095 cases • 1 µg/ml pronase E in modified HTF with 0.5% BSA 24 hours before ET • Prize paper 53rd ASRM 1997 34.6% BAH group Control group 29.3% Clinical preg. rate
premordial immature mature Ovary : Immature oocytes Uterus : Midproliferative endometrium implantation ↓ ovulation ↓ mense Suggested scheme of immature oocyte program In vitro maturation Immature oocyte retrieval Fertilization by ICSI Embryo development E2 (6 mg/day) Biochemical assisted hatching Proliferative endometrium hCG (10000 IU) Progesterone (50 mg/day) Embryo transfer Secretary endometrium Implantation
Endometrial preparation in IVM-IVF-ET Progesterone 50mg/day E2V 6mg/day Mense #1 OPU BAH UET ICSI hCG Regular mense Mid follicular phase 5,000 IU PCO Endometrial 10,000 IU thickness > 8mm
LH peak Implantation Endometrium Re-establishment 2PN Hatching Natural cycle 10 14 21 M #1 (windows) Ovu. 2PN Fert. Endometrium Re-establishment 20 Hatching IVM-IVF cycle 7 M #1 Day of OPU ICSI ET Implantation (?) hCG E2 (6 mg/day) P4 (50 mg/day) Implantation windows : Natural cycle vs. IVM-IVF cycle
Maturation rate of porcine immature oocytes with coculture of CHO cells Media Culture GV -> M II Porcine immature oocytes IVM media 24 hrs 34.4 % Growth media 24 hrs CHO * coculture 8.7 % CHO (-) 0.0 % Growth media + IVM media CHO coculture 48 hrs 52.4 % CHO (-) 48 hrs 43.5 % * CHO : Chinese Hamster Ovary cells
Overall results of IVM-IVF-ET in conparison with convertional ICSI-IVF-ET Convertional IVM-IVF-ET COH-ICSI IVF-ET Regular mense group PCO group No. of retrieved 11.0 ± 0.4 * 6.7 ± 0.4 13.6 ± 2.3 oocytes Maturaltion (%) 87.1 62.5 69.5 Normal fertilization 67.0 72.0 72.5 (%) Cleavage (%) 84.5 87.9 89.9 Pregnancy / transfer 34.2 16.9 28.3 (%) * Mean ± SEM
Conclusion • Minal ovarian stimulation - Efficiency in producing a healthy singleton pregnancy - Less complex, shorter stimulation, less risk & complications - Improved embryo selection and endometiral receptivity • IVF-IVF-ET - To get more healthy oocytes and embryos - To get more synchronized endometrium for implantation - To improve pregnancy rate
IVM baby 이다은 1998. 5. 25. 이은빈 2000. 10. 9.
Embryo-Maternal communication hCG endometrium EGF, LIF other cytokines hCG receptor ? embryo hCG Implantation good embryo good endometrium = x