Download
1 / 28
290 likes | 566 Views
EPILEPSY &THE DENTAL PATIENT. NEUROGENIC DISORDER (EPILEPSY). Neurogenic disorder of the brain. Epilepsy: Is the most common neurogenic disorder the dentist may face in his clinic. Potential problems: Precipitation of the attack.

E N D
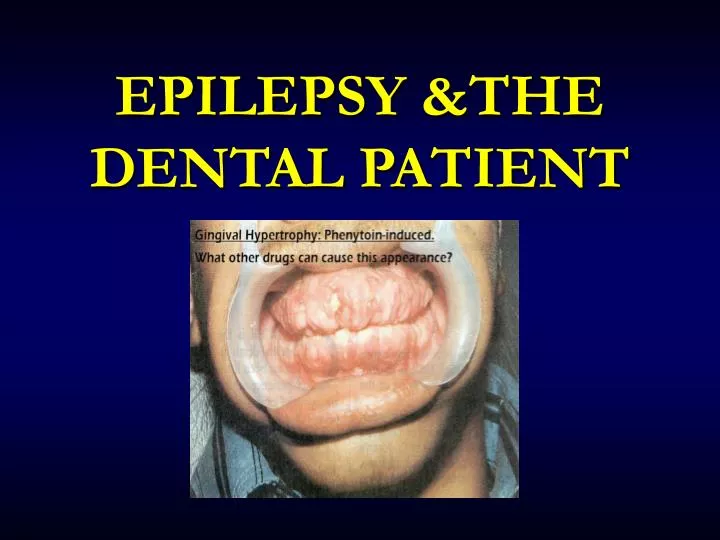
NEUROGENIC DISORDER (EPILEPSY) Neurogenic disorder of the brain. Epilepsy: Is the most common neurogenic disorder the dentist may face in his clinic. Potential problems: • Precipitation of the attack. • Problems of drugstaken a) Phenytoin------- Gingival hyperplasia b) Valproate------- Bleeding tendancy
Manifestations of Seizure Attack: • Isolated, brief seizure - Tonic-clonic movement of trunk & extremities - Loss of consciousness - Vomiting - Airway obstruction - Loss of urinary & anal sphincter control • Repeated or sustained seizure (Status Epileptics)
Epileptic Seizures • A neurologic disorder characterized by Recurrent Episodes of Seizures. • Grand mal seizure: Temporary loss of consciousness accompanied by uncontrollable muscular contractions and relaxation. • Phase 1: Aura • Phase 2: Loose consciousness • Phase 3: Muscle contractions • Phase 4: Sleep/recovery • Petit mal seizure: Brief lapse of consciousness that may last only a few seconds.
Definition: the clinical manifestation of an abnormal and excessive excitation of a population of cortical neurons Incidence: approximately 80/100,000 per year Lifetime prevalence: 9% (1/3 benign febrile convulsions) Seizures vs Epilepsy Seizures Epilepsy • Definition:a tendency toward recurrent seizures unprovoked by systemic or neurologic insults • Incidence:approximately 45/100,000 per year • Point prevalence: 0.5-1% • 14 years or younger 13% • 15 to 64 years 63% • 65 years and older 24% • Cumulative risk of epilepsy through 74 years old: 1.3% - 3.1%
Seizure vs Epilepsy Seizures Nonepileptic Epilepsy (Recurrent Seizures) Cardiovascular Drug related Syncope Metabolic (glucose, Na, Ca, Mg) Toxic (drugs, poisons) Infectious Febrile convulsions Pseudoseizure Alcohol/drug withdrawal Substance abuse Psychiatric disorders Sleep disorders (cataplexy) Idiopathic (primary) Symptomatic (secondary)
Questions Raised by a First Seizure Seizure or not? Focal onset? Evidence of inter - ictal CNS dysfunction? Metabolic precipitant? Seizure type? Syndrome type? Start AED?
Epilepsy • Definition: a state of recurrent seizures, not due to an identifiable metabolic cause • May be due to underlying genetic or congenital factors or to cerebral insult prenatally or later in life • Background: • 1 – 2% of the general population has seizures • Primary • Idiopathic epilepsy: onset ages 10-20 • Secondary • Precipitated by one of the following: • Intracranial pathology • Trauma, Mass, Abscess, Infarct • Extracranial Pathology • Toxic, metabolic, hypertensive, eclampsia
Types of Epilepsy 1- Partial Seizures -Simple partial seizure -Complex partial (Psychomotor) seizure 2.Generalized Seizures - G. Absence seizure (Petit mal) -Generalize tonic-clonic seizure (Grand mal)
Seizure Types • Generalized Convulsive Seizures (Grand Mal): • Tonic , clonic movements, (+) LOC, apnea, incontinence and a post ictal state • Non Convulsive Seizures (Petit Mal) • Absence seizures – “blank staring spells” • Myoclonic – brief contractions of selected muscle groups • Partial Seizures • Characterized by presence of hallucinations • Simple = somatic complaints + no LOC • Complex = somatic complaints + AMS or LOC
Epilepsy Precipitants • What might cause an otherwise stable patient to have a seizure? • Forgetting to take anticonvulsant • Stress –Emotional/Physical • Sleep disturbance • Hypoglycaemia • Alcohol withdrawal • Other medications • Anticonvulsants – withdrawal from – esp. benzodiazepines • Antidepressants • Antipsychotics • Antihistamines • Antibiotics • CNS stimulants • Theophylline, caffeine, cocaine, amphetamine • Nonsteroidal anti-inflammatory agents • Opiates
First Aid - Tonic-Clonic Seizure Turn person on side with face turned toward ground to keep airway clear, protect from nearby hazards Transfer to hospital needed for: • Multiple seizures or status epilepticus • Person is pregnant, injured, diabetic • New onset seizures DO NOT put any object in mouth or restrain
ANTIEPILEPTIC DRUGS 2nd Generation 1st Generation • Gabapentin • Lamotrigine • Topiramate • Tiagabine • Oxcarbazepine • Levetiracetam • Zonisamide • Pregabalin • Phenytoin • Carbamazepine • Sodium Valproate • Phenobarbital • Primidone
Approach for 1st Seizure, New Seizure, or Substance/ Trauma Induced Seizure • As always ABC’s First • IV, O2, Monitor. • Send blood for CBC, Chem, Tox screen as appropriate • Anticonvulsant levels • Prolactin levels / Lactate levels • For seizures that are prolonged—i.e. longer than 5 minutes or that re-occur without the patient regaining normal consciousness – Rx with: • Lorazepam • Is patient still seizing? Post ictal? Pseudoseizure? • Complete History and Physical Exam • Including detailed Neuro Exam • Repeat Neuro evaluations a must!
Medical Treatment of First Seizure(s) • Whether to treat first seizure is controversial ? • 16-62% will recur within 5 years • Relapse rate for second seizure is reduced by AEDs, • BUT long term prognosis of whether the patient will have refractory epilepsy is not • Increased risk of relapse • Abnormal imaging • Abnormal neurological exam • Abnormal EEG • Family history of epilepsy • Currently, most patients are not treated for the first seizure unless there is an increased risk for relapse
After seizure attack Patient Unconscious Patient Conscious • Place on side and suction airway • Monitor vital signs • Initiate BLS • Administer O2 • Prepare to ER • Suction airway • Monitor vital signs • Administer O2 • OBSERVE for at least 1hr and consult physician If sustained • Diazepam 5mg/min IV • Midazolam 3mg/min IV or IM • Phenytoin10~15mg/kg IV
Prevention of Peri-operative Seizures • Patients must take their anticonvulsant medication • If general anaesthetic – anaesthetist should be aware of seizure tendency • Check patient’s pre-operative anticonvulsant levels • Consult with patient’s neurologist or family physician • Most stable epileptics, well-controlled on medication, can undergo surgery without difficulty or complication
Dental treatment of the Epileptic patients AEDs 2. Adequate history -Nature of seizure -Seizure control -Medication compliance 1. Patient handling -Chair position -Patient’s head -False teeth 3. Treatment planning -Stressful situation -Photic stimulation -Hypoglycemia 4. Education - dental staff
2. Signs of liver damage 3. Signs of lymphadenopathy Stevens-Johnson syndrome 4. Cosmetic effects: hirsutism, coarsening of face, widening of jaws, thickening of lips Dental practice & AED 1. Unexplained oral manifestations eg. mucosal bleeding, sore tongue or mouth, ulcerations in the mouth, Blood dyscrasias; aplastic anemia, Agranulocytosis, Thrmbocytopenia
-Stevens-Johnson syndrome Stevens-Johnson syndrome (valproate), nausea, ataxia Valproate & Lamotrigine
Status Epilepticus Definition • Operationally defined as seizure lasting greater than 5 minutes OR two seizures between which there is incomplete recovery of consciousness. • “Recurrent seizures with failure to recover from one seizure before next seizure begins”
Status Epilepticus A medical emergency • Adverse consequences can include hypoxia, hypotension, acidosis and hyperthermia • Goal: stop seizures as soon as possible • Hypertension (early) • Arrhythmias • Neurogenic • Hypotension (late) • Aspiration • Injury, burns etc • Hypoxia • Lactic acidosis • Hypercarbia • Rhabdomyolysis • Hyperpyrexia • Hypoglycaemia
Aetiology • Tumour • Cerebrovascular disease • Head injury • Infection • Hypoxic encephalopathy • Drug abuse / overdose / withdrawal • Metabolic • Primary epilepsy • Pseudoepilepsy
Treatment • ABC & oxygen & IV access • Glucose if indicated or unsure (50mls/D50 • Diazepam or lorazepam IV (or PR) • Phenytoin (to terminate SE or prevent further fits) • Monitor ECG and BP • Investigate & monitor (EEG) • Persistent: > Further phenytoin > Phenobarbitone > Thiopentone Propofol
Prognosis Depends on • Aetiology • Age • Duration of status • Systemic complications (anoxia) • Treatment given Mortality: 3 – 35%
After seizure attack Patient unconscious Patient conscious • Place on side and suction airway • Monitor vital signs • Initiate BLS • Administer O2 • Prepare to ER • Suction airway • Monitor vital signs • Administer O2 • OBS for at least 1hr and consult physician If sustained • Diazepam 5mg/min IV • Dormicum 3mg/min IV or IM • Dialantin 10~15mg/kg IV