Download
1 / 39
390 likes | 530 Views
Attachment D. Faculty Group Practice Clinical Strategy 2010-2015. FGP Board July 09, 2009. Brief Background of Faculty Group Practice. 1970’s Departmental practice plans created within the medical school 1984 Clinics and ancillary services become hospital based

E N D
Attachment D Faculty Group PracticeClinical Strategy2010-2015 FGP Board July 09, 2009
Brief Background of Faculty Group Practice 1970’s Departmental practice plans created within the medical school 1984 Clinics and ancillary services become hospital based 1995 Medical Center Clinicians Group formed to improve the delivery of clinical care 1996 Faculty Group Practice created 2008 FGP Board reorganized to include all chairs, faculty representatives, and health system executives 2008 FGP assumes responsibility for Ambulatory Care Services FGP Board July 09, 2009
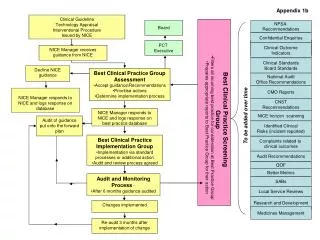
University of Michigan Medical School Faculty Group Practice (FGP) Organizational Structure Committees Budget & Finance Committee Clinical Practice Committee Executive Committee Nominating & Bylaws Committee Dean (Chair of Board) Board of Directors Executive Hospital Director Sr. Associate Dean for Clinical Affairs Contracting Chief Administrative Officer Administrator, Ambulatory Care Services ACOC Ambulatory Surgery BODT JCAHO Programs Property Systems Professional Compliance Compliance Program Q.A. Training Education Quality Management Center BCBSM PGIP Complex Care Disease Mgt. CMS Demo Kids Connection Outcomes Analysis Project Mgt. Director of Billing Customer Service IDX MCA Payor Relations PBAC Training Health System Finance Support Budgeting Capitation Funds Management Financial Planning Financial Reporting Modeling Venture Funds Management FGP Board July 09, 2009
FGP Board of Directors FGP Board July 09, 2009
Goals of Reorganization/HHC-FGP Agreement of 2008 Improve clarity of management of clinical practice, clinics and ancillary support Promote local problem solving Increase faculty compensation to benchmark Improve coordinated planning and decision making Enhance implementation of initiatives Improve strategic planning FGP Board July 09, 2009
Elements of HHC-FGP Agreement/Board Reorganization FGP assumes responsibility for managing ambulatory services on behalf of HHC FGP assumes financial risk, shares margin improvement 50:50 with HHC HHC provides $17 million/year for faculty salary support HHC funds capital Clinical chairs, 5 at-large faculty, hospital and medical school leadership – comprise Board FGP Board July 09, 2009
Results to Date Faculty salary gap reduced from $29 million to $14 million FY09 Patient satisfaction up to 87.6 (90 goal) Medical directors appointed for each clinic and ancillary area (ACU) Margin improvement YTD (May) - $8.5 million Incentives created for patient access, patient satisfaction, improved coordination Medical directors/managers – professional development Monthly management information provided to each Ambulatory Care Unit (ACU) Increased transparency FGP Board July 09, 2009
Medical School Faculty Satisfaction Survey – Clinical Activities, Fall 2008 Patient Care and Clinical Activities20062008 Clerical Support in the clinic 60.5 66.5 Nursing support in clinical activities 65.5 70.0 Support provided by medical assistants 67.7 71.6 Timeliness of diagnostic tests & procedures 62.3 69.0 Timeliness of the transcriptions 79.7 82.8 Patient scheduling in clinic 55.5 62.0 FGP Board July 09, 2009
Faculty Group Practice Strategic Planning Began in Fall 2008 FGP defines clinical strategy Based on 2008 Harvard Business Review article – Can You Say What Your Strategy Is?By David Collis and Michael Rukstad FGP Board July 09, 2009
Components of Clinical Strategy Competitive Advantage – Excellent faculty Scope or Focus – Nationally recognized faculty and clinical programs 5 year goal Double Clinical Research (number of patients accrued to clinical trials) Patient satisfaction greater than 90 in all areas Referring physician satisfaction > 90 National leader in quality and safety FGP Board July 09, 2009
Mission The mission of the FGP is to manage the clinical enterprise of the medical school clinical faculty for the benefit of education, research and patient care programs of the University of Michigan. FGP Board July 09, 2009
Vision The national leader in clinical quality, safety and innovation. FGP Board July 09, 2009
Clinical Strategy Statement of the FGP The focus of the FGP will be to provide exemplary clinical care and service to our patients, develop nationally recognized faculty and clinical programs and increase clinical research, doubling clinical research by 2015. FGP Board July 09, 2009
Goal 1: Exemplary Clinical Care and Service A. Engage medical directors, Clinical Practice Committee, faculty, nursing, and clinic staff to improve clinical care and service with the following goals Improve patient satisfaction >90 in all clinics Improve referring satisfaction >90 in all departments Improve access for new patients >80% in <4 weeks Improve coordination of care between dependent services B. Improve Efficiency Train medical directors and managers in techniques to solve problems, streamline processes (Lean) Provide central resources to facilitate problem solving (Coaches) Strive for 5% productivity gain each year for the period 2010-2015 FGP Board July 09, 2009
Goal 1 – continuedExemplary Clinical Care and Service C. Improve Quality of Care Develop and measure process and outcomes in all service areas Implement E-Prescribing Implementation of disease management/preventative software Complex Care Management Program will focus on high cost at risk populations Incorporate outside lab tests into CareWeb – improve continuity Measure the quality of our care in all disciplines Continue Guideline Development for problem areas (pain management, imaging utilization) Display our quality measures for public viewing FGP Board July 09, 2009
Goal 2: Develop Nationally Recognized Faculty and Clinical Programs A. Utilize destination program process to focus our resources Implement current approved programs using existing operations Proceed with second round of programs Utilize lean techniques to streamline processes Improve faculty mentorship and support Improve clinical research infrastructure support Close salary gaps in departments Streamline IRB process C. Targeted recruitment to support destination program development and research strategic plan (under development) FGP Board July 09, 2009
Goal 3: Double Clinical Research by 2015 Engage research and regulatory/compliance office to streamline processes (billing calendar, IRB process, clinical design support) Engage departments to understand barriers to increasing clinical research FGP – margin will support clinical research FGP Board July 09, 2009
Next Steps Chairs discuss with faculty Faculty representative discuss with cohort FGP leadership will work with ACU leadership to develop 2-3 goals for 2010 Track progress in FGP Board quarterly FGP Board July 09, 2009
Measures for FGP Board Measure for clinical research Access report card Patient satisfaction National reputation? FGP Board July 09, 2009