Download
1 / 45
500 likes | 1.73k Views
Safety; Basic Body Mechanics; Moving & Positioning. Nursing 125. Patient Safety:.

E N D
Safety; Basic Body Mechanics; Moving & Positioning Nursing 125
Patient Safety: • “Technically the biggest ‘safety system’ in healthcare is the minds and hearts of the workers who keep intercepting the flaws in the system and prevent patients from being hurt. They are the safety net, not the cause of injury”. Don Berwick
Patient Safety #1 • A client’s health and wellness depend upon safety. Safety is the number 1 priority in all aspects of care. • Nurses need to be aware of safety. The hospital setting is complex, potentially dangerous & unfamiliar to clients.
Ensuring Client safety: • Reduces length of stay & cost of treatment • Reduces frequency of treatment • Reduces potential for law suits • Reduces the number of work-related injuries to personnel
Institute of Medicine Report, 1999 • Estimated 48,000-98,000 deaths per year from medical errors. • Adverse events ranked as the 8th leading cause of death, ahead of MVA’s, breast cancer and AIDS • Extrapolating from the U.S. data, adverse events would account for 4,000-10,000 deaths per year in Canada.
Impetus for action: Threefold 1. Health system has a moral imperative to ensure the safety of patients • Adverse events have a tremendous cost to the system in extended hospital stays & additional medical procedures • Adverse events expose health organizations to legal liability
A safe environment is one in which basic needs are met, physical hazards are reduced or eliminated, transmission of organisms is reduced and sanitary measures are carried out.
Falls • Fall risk, especially in the elderly, is growing. In hospitalized patients, 4-12 falls occur per 1,000 bed days, ranking them among the 10 most common claims presented to insurance agencies Nursing Management, September 2002 • 30% of people 65 yrs and older (in the community) fall at least once each year.
Focus Assessment: • To ensure patient safety – the nurse should conduct a focus assessment during every nurse-patient encounter which includes: • A visual scan of the environment for potential hazards • A quick appraisal of patient related factors
Strategies to help reduce falls: Physical environment • Appropriate furniture and lighting • Call bell easily accessible/personal items within reach • Traffic areas free from obstruction • Secure/remove loose carpets or runners • Eliminate clutter • Grab bars in appropriate areas in washroom • Handrails in the halls • Keep bed in a low position – lock bed/wheelchairs/stretcher • Identify clients at risk for falls. • If a client experienced falls at home, they will likely continue to be at risk for falls in the hospital setting. Place them close to nsg station.
Strategies to help reduce falls: (Communication/Assessment) • Orient client to physical surroundings • Explain use of call bell • Assess client’s risk for falling • Alert all personnel to the client’s risk for falling • Instruct client and family to seek assistance when getting up • Maintain client’s toileting schedule • Observe/assess client frequently • Encourage family participation in client’s care
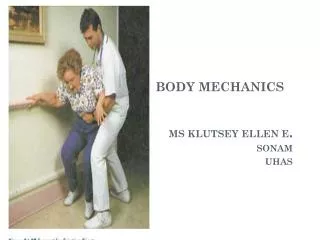
Body Mechanics • The coordinated efforts of the musculoskeletal & nervous system to maintain balance, posture & body alignment during lifting, bending, moving & performing ADL’s. • Knowledge & practice of proper body mechanics protect the client and nurse from injury to their musculoskeletal systems. • Correct body alignment reduces strain on musculoskeletal structures, maintains muscle tone, & contributes to balance.
Body Mechanics (cont.) • Body balance is achieved when a wide base of support exists, the center of gravity falls within the base of support & a vertical line can be drawn from the center of gravity through the base of support. • When lifting an object, come close to the object, enlarge the base of support & lower the center of gravity.
Body Mechanics (cont.) • Proper body mechanics facilitates movement without muscle strain & excessive use of muscle energy. • Improper body mechanics can lead to injury for both the nurse & the patient, especially back injury when lifting.
“In 1990, Canadian hospitals reported 30,487 time loss injuries. Fifty-three percent were sustained by nurses. Almost half (of the injuries) were back injuries. Back injury is now recognized as one of the major reasons for ill-health retirement from nursing. Not only is it the most frequent injury sustained by nurses, it is the most debilitating”
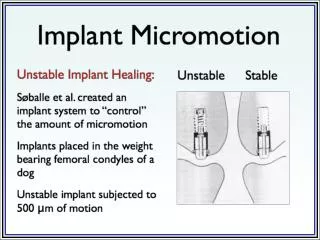
Moving & Positioning Mobility – persons ability to move about freely. Immobility – person unable to move about freely, all body systems at risk for impairment. • Frequent movement improves muscle tone, respiration, circulation & digestion. • Proper positioning at rest also prevents strain on muscles, prevents pressure sores (decubitus ulcers within 24 hours) & joint contractures (abnormal condition of a joint, characterized by flexion & fixation & caused by atrophy & shortening of muscle fibers or by loss of normal elasticity of the skin).
Moving & Positioning (cont.) • Pressure Sores – tissues are compressed, decreased bld supply to area, therefore, decreased oxygen to tissue & cells die.
Correct Positioning • Is crucial for maintaining body alignment and comfort, preventing injury to the musculoskeletal system, and providing sensory, motor, and cognitive stimulation. • It is important to maintain proper body alignment for the patient at all times, this includes when turning or positioning the patient. • Aim – least possible stress on patient’s joints & skin. Maintain body parts in correct alignment so they remain functional and unstressed. • Patients who are immobile need to be repositioned q 2 hrs.
Application of proper body mechanics “By applying the nursing process and using the critical thinking approach, the nurse can develop individualized care plans for clients with mobility impairments or risk for immobility. A care plan is designed to improve the client’s functional status, promote self care, maintain psychological well being, and reduce the hazards of immobility.”(Potter and Perry, 2006)
Moving & Positioning: Nursing Process • Assessment • Comfort level & alignment while lying down • Risk factors - Ability to move, paralysis • Level of consciousness • Physical ability/motivation • Presence of tubes, incisions, equipment • Nursing Diagnosis • Defining characteristics from the assessment • Activity intolerance • Impaired physical mobility • Impaired skin integrity refer to Perry and Potter
Nursing Process (cont.) • Planning • Know expected outcomes – good alignment, increased comfort • Raise bed to comfortable working height • Remove pillows & devices • Obtain extra help if needed • Explain procedure to client • Implementation • Wash hands • Close door/curtain • Put bed in flat position • Move immobile patient up in bed • Realign patient in correct body alignment (pillows etc.)
Nursing Process (cont.) • Evaluation • Assess body alignment, comfort • Ongoing assessment of skin condition • Use of proper body mechanics (nurse)
Restraints • Device used to immobilize a client or an extremity • A temporary means to control behavior • Restraints are used to: • Prevent falls & wandering • Protect from self-injury (pulling out tubes) • Prevent violence toward others • Restraints deprive a fundamental right to control your own body.
CRNNS Position Statement on Use of Physical Restraints • “The Registered Nurses’Assoc. of N.S. recognizes the right of all persons to be treated in a respectful and dignified manner. Additionally, the CRNNS believes that all individuals have an inherent right to autonomously and independently make decisions regarding their health care. (RNANS, 1997) • Use of physical restraints may violate these inherent rights. • The CRNNS does not endorse the use of physical restraints.
Cautious Use of Restraints • While restraint-free care is ideal, there are times that restraints become necessary to protect the patient & others from harm. • Highly agitated, violent individual – Physical/Chemical restraints • Intubated patient – pulling out endotracheal tube • Suicide patient - ? Chemical restraints
Use of Restraints: • Use only when absolutely necessary. • Attending physician is responsible for the assessment, ordering & continuation of restraint. • Can be instituted on your nsg judgment – must have a doctors order ASAP. • Continued use of restraints must be reviewed daily by the RN & documented on the health record. • Always explain what you do & why, to reduce anxiety & promote cooperation.
Goals of Restraint Use • To avoid the use of restraints whenever possible. • Encourage alternatives • Family member to sit with patient • Geri chair vs. bed • Non restraint measures – safety belt, wedge pillows, lap tray • Consider restraints as a temporary measure – decrease likelihood of injury from restraint use. • Remove restraints as soon as the patient is no longer at risk for injury.
Complications assoc. with restraints • Hazards of immobility • Death • Pressure sores, pneumonia, constipation, incontinence, contractures, decreased mobility, decreased muscle strength, increased dependence • Altered thought processes • Humiliation, fear, anger & decreased self-esteem • Strangulation • Compromised circulation • Lacerations, bruising, impaired skin integrity • Must release restraint every 2 hours for assessment & ROM
Physical Restraints – device that limits a clients ability to move • Side rails – stop patient from rolling out, but does not stop them from climbing out – side rail down when working on that side. • Jackets & Belts – patient who is confused & climbing over rails may need a jacket or belt to restrain them to bed. Sleeveless with cross over ties, allows relative freedom in bed. • Arm & Leg – Undesirable, limits patients movement, injury to wrist/ankle from friction rubbing against skin – use extra padding. Restrain in a slightly flexed position, if too tight could impair circulation. Never tie to a bed rail.
Physical Restraints (cont.) • Mitts are used for those confused & pulling at@ edges of dsgs, tubes, iv’s, wounds. Doesn’t limit arm movement, soft boxing glove that pads the hand, remove, wash & exercise. • Ensure not too tight • Use quick release tie for all restraints
Chemical Restraints • Medication • Patient must be closely observed and assessed frequently post medication. • Remains a high risk for injury.
Supporting Documentation • Rationale for the use of restraints, including a statement describing the behavior of the patient. • Previous unsuccessful measures or the reason alternatives are not feasible. • Decision to restrain with the type of restraint selected and date & time of application. • Observations regarding the placement of the restraint, its condition and the patient’s condition, including the frequency of observation (not just at the end of your shift)
Supporting Documentation (cont.) • Assessment of the need for ongoing application of restraint. • Care of the patient which may include re-positioning, toileting, mobilization and/or skin care
Civil Actions • Most civil cases are based on allegations of negligence. • Important to support your judgment/actions with quality documentation
Promoting Safety • Measures designed to promote client safety are the result of individualized assessment findings. Often it is the conclusion of the nurse that a client’s safety is at risk, and subsequent nursing interventions are implemented. Assessment of a client’s safety should occur in the home, healthcare facility, and community environment. (Perry and Potter, 2002)
Canadian Nurses Association’s (CNA) online Patient Safety Resource Guide • www.cna-aiic.ca
Nursing 125 LAB Safety; Basic Body Mechanics; Moving & Positioning
Tips for positioning the patient • After turning – use aids i.e. pillows, towels, washcloths, blankets, sandbags, footboards etc. • Joints should be slightly flexed b/c prolonged extension creates undue muscle tension & strain • Supine • Low or flat pillow (prevents neck flexion) • Trochanter role (supports hip joint prevents external rotation) • Hand roll – used if hands are paralyzed (thumb & fingers flexed around it) • High top sneakers, foot board, sandbags (support feet with toes pointing upward. Prolonged plantar flexion leads to foot drop (permanent plantar flexion & inability to dorsiflex)
Tips (cont.) • Side lying • Even if paralyzed on one side a patient can be placed on that side. Take care not to pull on the affected extremity. • Head on low pillow, pillow along back – supports back & holds body in position, underlying arm comes forward & flexed onto pillow used for head, top arm flexed forward & resting on pillow in front of body, hand rolls if necessary, flex top leg forward & place on pillow, feet at right angles with sandbag.