Download
1 / 1
10 likes | 326 Views
“The Pen Is Mightier Than The Sword.” Drug Chart Documentation In Care Of The Elderly . Jegatheesan M, Sandhu JK and Lo H. Care of the Elderly , Kingston Hospital Trust NHS. mjegat@doctors.co.uk. Objective. Results. Recommendations .

E N D
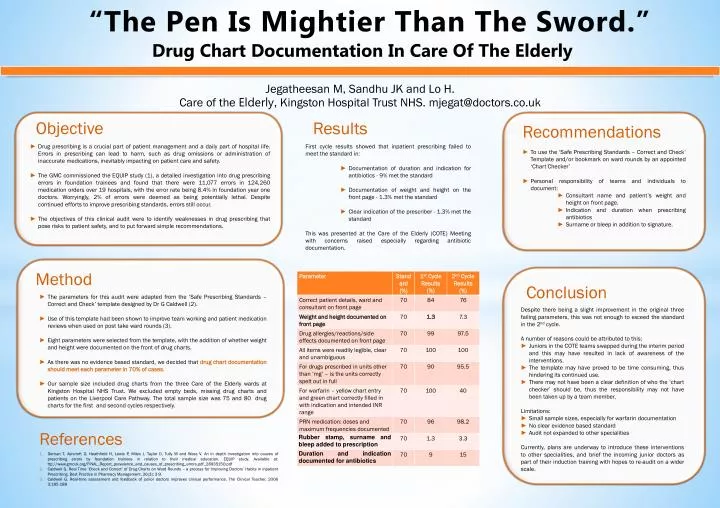
“The Pen Is Mightier Than The Sword.” Drug Chart Documentation In Care Of The Elderly Jegatheesan M, Sandhu JK and Lo H. Care of the Elderly, Kingston Hospital Trust NHS. mjegat@doctors.co.uk Objective Results Recommendations • Drug prescribing is a crucial part of patient management and a daily part of hospital life. Errors in prescribing can lead to harm, such as drug omissions or administration of inaccurate medications, inevitably impacting on patient care and safety. • The GMC commissioned the EQUIP study (1), a detailed investigation into drug prescribing errors in foundation trainees and found that there were 11,077 errors in 124,260 medication orders over 19 hospitals, with the error rate being 8.4% in foundation year one doctors. Worryingly, 2% of errors were deemed as being potentially lethal. Despite continued efforts to improve prescribing standards, errors still occur. • The objectives of this clinical audit were to identify weaknesses in drug prescribing that pose risks to patient safety, and to put forward simple recommendations. • First cycle results showed that inpatient prescribing failed to meet the standard in: • Documentation of duration and indication for antibiotics - 9% met the standard • Documentation of weight and height on the front page - 1.3% met the standard • Clear indication of the prescriber - 1.3% met the standard • This was presented at the Care of the Elderly (COTE) Meeting with concerns raised especially regarding antibiotic documentation. • To use the ‘Safe Prescribing Standards – Correct and Check’ Template and/or bookmark on ward rounds by an appointed ‘Chart Checker’ • Personal responsibility of teams and individuals to document: • Consultant name and patient’s weight and height on front page. • Indication and duration when prescribing antibiotics • Surname or bleep in addition to signature. Method Conclusion • The parameters for this audit were adapted from the ‘Safe Prescribing Standards – Correct and Check’ template designed by Dr G Caldwell (2). • Use of this template had been shown to improve team working and patient medication reviews when used on post take ward rounds(3). • Eight parameters were selected from the template, with the addition of whether weight and height were documented on the front of drug charts. • As there was no evidence based standard, we decided that drug chart documentation should meet each parameter in 70% of cases. • Our sample size included drug charts from the three Care of the Elderly wards at Kingston Hospital NHS Trust. We excluded empty beds, missing drug charts and patients on the Liverpool Care Pathway. The total sample size was 75 and 80 drug charts for the first and second cycles respectively. • Despite there being a slight improvement in the original three failing parameters, this was not enough to exceed the standard in the 2nd cycle. • A number of reasons could be attributed to this: • Juniors in the COTE teams swapped during the interim period and this may have resulted in lack of awareness of the interventions. • The template may have proved to be time consuming, thus hindering its continued use. • There may not have been a clear definition of who the ‘chart checker’ should be, thus the responsibility may not have been taken up by a team member. • Limitations: • Small sample sizes, especially for warfarin documentation • No clear evidence based standard • Audit not expanded to other specialities • Currently, plans are underway to introduce these interventions to other specialities, and brief the incoming junior doctors as part of their induction training with hopes to re-audit on a wider scale. References • Dornan T, Ashcroft D, Heathfield H, Lewis P, Miles J, Taylor D, Tully M and Wass V. An in depth investigation into causes of prescribing errors by foundation trainees in relation to their medical education. EQUIP study. Available at: ttp://www.gmcuk.org/FINAL_Report_prevalence_and_causes_of_prescribing_errors.pdf_28935150.pdf • Caldwell G. Real Time ‘Check and Correct’ of Drug Charts on Ward Rounds – a process for Improving Doctors’ Habits in Inpatient Prescribing. Best Practice in Pharmacy Management. 26(3): 3-9. • Caldwell G. Real-time assessment and feedback of junior doctors improves clinical performance. The Clinical Teacher. 2006 3;185-188